Recovery after a stroke
It will definitely not be easy, but the result is worth all the effort. We will gladly and readily participate in your rehabilitation with useful information and practical advice.
Recovery after a stroke is a thorny path, but all doctors strongly recommend starting it with a complex
physical exercises aimed at restoring fine motor skills of the fingers and toes. Why specifically with motor skills? Because it has been proven that various exercises for the fingers help to activate the work of the brain, which suffered the heaviest blow from the stroke and which is responsible for the sensitivity and motor activity of the limbs (it is generally responsible for everything). With the help of a set of exercises for the fingers and toes, an extremely important relationship is created:
- Fingers are developed - the brain is activated
- Brain function improves - sensitivity of the limbs is restored
The set of exercises below must be performed regularly - 3-4 times a day. This is the main condition for returning to normal life. If a limb is completely paralyzed, have someone move your fingers.
And further. Even if at first you don’t succeed, under no circumstances stop practicing. Believe in yourself and your body. Be persistent, patient and optimistic. You will definitely succeed!
Prescription of exercise therapy after ischemic stroke
In addition to disturbances in brain functions to control body movement, all patients are faced with the results of prolonged immobility. These consequences are especially threatening for elderly, overweight patients who were already inactive.
The starting points for restoring motor activity are massage and physiotherapy. In the future, after the mobility of the limbs has returned, sets of exercises are prescribed, which can be performed in a lying, sitting, or standing position.
The purpose of the classes is:
- prevention of muscle atrophy;
- fight against bedsores, blood clots;
- prevention of pneumonia, pulmonary congestion;
- help the cardiovascular system;
- removal of muscle tone.
While the patient cannot perform the actions himself, he should be helped by specialists and relatives.
Important: Passive exercises help preserve muscle memory and make it easier to act independently as your condition improves.
Restoring finger sensitivity
1. Carefully, over the entire area, with medium force/pressure, knead each finger of the affected limb. Spend about 20-30 seconds on each finger.
2. In a sitting position, place your hands, palms down, on your thighs, spread your fingers. Simultaneously on both hands, in turn, raise your fingers. Start with the thumb and end with the little finger, lower the fingers and do the same in reverse order, starting with the little finger. Do the exercise 10 times (if it doesn’t work out well, increase the number of repetitions).
Then turn your hands over with your palms up and do the exercise 10 more times. If you find it difficult to sit, practice lying down with your hands on your chest or stomach (it is advisable that you can see them). The same exercise can be used for your toes.
3. Difficult even for healthy people, but extremely useful and important for activating the brain: place your hands on your hips or chest/stub with your palms down, fingers slightly apart. At the same time, on both hands, in turn, turn each finger first in one direction and then in the other direction. Repeat 5-7 times. Turn your hands over with your palms facing up and repeat the exercise.
4. Spread the fingers of both hands as synchronously as possible, hold it there for a little while and clench it into a strong fist for 10 seconds. Repeat at least five times. Do a similar exercise for your toes: spread them out, and then bend them down, squeezing them tightly so that they touch the sole of your foot.
5. Exercise for your toes: pull your toes towards you and spread them as far apart as possible, then away from you and squeeze (pull your toes). Do the exercise 10 times.
6. Clasp your hands and lift the fingers of the same name one by one (thumb of the right hand, then the thumb of the left, index finger on the right, then on the left, etc.). Then do all this in reverse order. Repeat 10 times.
7. Imagine that you click someone on the forehead (give a click), and alternately use different fingers: thumb and index, thumb and middle, thumb and ring, thumb and little finger, and then in reverse order. Do 5 repetitions for each hand (can be synchronized or in turn).
8. Exercises with a special hedgehog massage ball. Squeeze it in your fist and between the fingers of both hands, throw it from hand to hand, massage your hands with it, roll it between your fingers - in general, for 3-5 minutes, actively do with it whatever your imagination tells you.
9. Take two small balls or walnuts in one hand and roll them in your palms. This can be done alternately for each hand or simultaneously for both (then you will need 4 balls or nuts). Practice for about 3-5 minutes.
10. Discover your talent as a sculptor and sculpt various small figures from plasticine or clay as much as possible.
How to restore sensory sensitivity in your hands
To restore sensory sensitivity in your hands, perform these exercises daily, several times a day (for some of them you will need an assistant).
1. Try to identify different textures by touch. Fabrics (silk, velvet, cotton, fur, etc.), surfaces of objects with different coatings (smooth, rough, smooth, bumpy, etc.), hard and soft materials, hard and elastic. In general, explore everything that is around you with your fingers, analyzing your sensations. First do this with your eyes open, and then with your eyes closed.
2. Hide several small objects (coin, cube, bead, shell, fruit pit, etc.) in a bowl of dry sand or some cereal and try to find and identify them by touch with your injured hand without the help of your eyesight. Or another task: feel some small object and hide it in the sand/grains along with other, unexplored objects - find it without the help of sight.
3. Take a soft plastic cup half filled with water in your sore hand. Hold it, lift it, place it on the table, and perform other manipulations. trying not to spill water or drop the glass. Let your vision help you in this matter: if you see that water is being squeezed out of the glass (pouring over the edges), reduce the squeezing force and, conversely, if the glass falls out of your hand, squeeze it harder.
4. Ask an assistant to apply a warm and cold object to the sore hand - analyze your sensations and ability to determine the temperature difference.
5. Close your eyes and ask an assistant to alternately place a light object in your sore hand, and then a much heavier object (preferably approximately the same size, so that there is no hint). Determine which one was lighter and which one was heavier. When you learn to clearly distinguish between the weights of these objects, complicate the task, gradually reducing the difference between the mass of objects. For this exercise, it is convenient to use kitchen scale weights.
What is a stroke
The brain is without a doubt the most important organ of the human body and it needs active nutrition and blood supply. Even such a phenomenon as fainting was “invented” by nature in order to ensure the flow of oxygen to the head - in a horizontal position.
The vessels of the brain, like the vessels of the whole body, wear out with age: this may be due to atherosclerosis - the appearance of cholesterol plaques that narrow the lumen of the arteries - or hypertension. If the pathological process develops slowly, then it leads to a gradual deterioration in the functioning of the nervous system: therefore, many older people develop vascular dementia, in which there is a deterioration in memory, attention, intelligence, changes in character, and so on.
If, under certain circumstances, a vessel in the brain becomes clogged, compressed or ruptured, then acute cerebrovascular accident occurs. This condition requires emergency medical care, which is aimed at eliminating the consequences of the attack and can save the patient's life or reduce the degree of damage to the nervous system.
Unfortunately, it is impossible to help a person who has had a stroke at home. Therefore, it is so important to recognize the signs of this condition and transport the patient to a specialized hospital as soon as possible.
Types of strokes
Depending on the mechanism of circulatory disorders, there are two main types of stroke:
- Ischemic stroke. It develops when the lumen of a vessel is blocked by an atherosclerotic plaque, thrombus (blood clot), air bubble, and so on. Another possible cause of ischemic stroke is a sudden drop in blood pressure, in which blood does not flow to a certain part of the brain. Strokes of this type are diagnosed in 80% of patients.
- Hemorrhagic stroke. It usually develops as a result of a sharp jump in blood pressure, which leads to rupture of a cerebral vessel, followed by hemorrhage into the soft tissue of the brain or the space between its outer membranes. According to statistics, a hemorrhagic stroke more often ends in the death of the patient: it requires emergency surgical care aimed at removing the hematoma compressing the brain.
Causes
Decreased sensitivity in the left half of the body (hemitype).
- The main and most common cause is ischemic stroke (IS), which occurs in the branches of the internal carotid artery (ICA). It is known that its branches participate in the blood supply to the cortex of the frontal, parietal and temporal lobes, the white matter of the subcortex, and the internal capsule. Hemihypesthesia (HH) occurs when the intracranial part of the ICA is blocked, combined with contralateral hemiparesis (changes in the motor sphere on the opposite side of the body).
- HHZ up to hemianesthesia (GAZ) occurs with infarctions in the branches of the middle cerebral artery (MCA), which is responsible for the blood supply to the cortex of the temporal and parietal lobes, subcortical nodes and internal capsule (IC). If the trunk of the MCA is affected in the area before the branches of the deep type depart from it, total IS appears, which, in addition to GAZ, is characterized by severe hemiplegia and hemianopsia (blindness of half the visual field on both sides). After the branches depart, similar manifestations form, but to a lesser extent.
- With strokes in the vertebrobasilar region , when the posterior inferior cerebellar artery (PICA) is blocked, Wallenberg-Zakharchenko syndrome develops, characterized on the affected side by pain and temperature hemihypesthesia of the face, cerebellar ataxia, Horner's syndrome (presence of ptosis, miosis, enophthalmos), pharyngeal paralysis, dysphagia , dysphonia, dysarthria, and on the opposite side – pain and temperature hemihypesthesia in the trunk and limbs, as well as dizziness, nausea and vomiting. This syndrome is one of the varieties of alternating syndrome that occurs with brainstem stroke. Hemihypesthesia (HH) in this case may be a thalamic type of sensitivity disorder, that is, it occurs with damage to the thalamus, or visual thalamus (a paired structure in the form of accumulations of gray matter, the main function of which is the transmission of information from sensory organs, except for the olfactory, to the corresponding areas of the cortex hemispheres), accounting for approximately 25% of all cases of vertebrobasilar strokes.
- If the small arterial branches of the brain are affected, a lacunar stroke (LI) develops, leading to pain and temperature-type HHS, which is called a “pure sensory microstroke.” Also, such manifestations can be combined with motor disorders when the posterior leg of the AC, the anterior leg or knee of the AC and the thalamus are affected (the so-called “sensorimotor microstroke”).
- In hemorrhagic stroke (HI) with hemorrhages in the basal ganglia (BG) and VC, GAS also appears in combination with a decrease or loss of muscle strength in half of the body - hemiplegia, hemianopia, paresis of the facial muscles and signs of changes in the dominant (aphasia) and subdominant (changes in the body diagram, autopathognosia and anosognosia) hemispheres. GAZ occurs with hemorrhages in the thalamic region, combined with hemiataxia, hemianopsia, amnesia, drowsiness and apathy.
What to do if there is a decrease in muscle strength in half of the body - hemiparesis, read here
Types of decreased sensitivity by hemitype
Characteristic is a decrease in sensitivity in the extremities of the half of the body opposite the lesion in the brain with a predominance of a decrease in its deep types (spatial sense of position of the body and limbs - muscular-articular; two-dimensional-spatial - determination of pressure and own body weight; vibration - the ability to perceive the action of vibrations ; and skin-kinesthetic – determining the direction of shifting of one’s own skin fold).
Moreover, such disorders usually arise against the background of hyperpathy (distortion of the threshold of perception, including pain: the patient cannot distinguish a cold object from a hot one, or a weak pain impulse causes severe pain).
Thalamic pain is burning, periodically intensifies and is generally difficult to treat
In case of damage to the sensory pathways of the posterior leg of the VC, contralateral HGZ or GAZ occurs.
In case of damage to the cerebral cortex of the brain, paresthesia occurs - feelings of tingling, crawling and numbness on one side of the upper lip, tongue, face, arm or leg, and they can occur in the form of focal sensory paroxysms.
If the trunk of the brain is affected, a disorder of surface sensitivity (pain, temperature and partially tactile) develops in an alternating type in the form of GAZ (for example, with stroke in the VBB - indicated above).
What is a microstroke?
In some cases, circulatory disorders in the brain are short-term in nature and go away on their own within 24 hours after the first symptoms of a stroke. Doctors call this condition a transient ischemic attack (TIA), but among ordinary people the term “ministroke” is popular.
Despite the fact that it does not threaten the patient’s life and in most cases does not entail serious health consequences, a microstroke requires mandatory examination by a neurologist, treatment and rehabilitation: 10% of patients develop a “full-fledged” stroke in the next 90 days after a TIA.
As a rule, an attack of cerebrovascular accident begins with a person’s complaints of acute pain in the head. It is important to know the main symptoms of a stroke, which doctors, for convenience, have combined into the acronym STROKE:
- S (smile) : Ask the person you suspect is having a stroke to smile. If at the same time the corner of the lip on one side remains drooping (or the whole face seems to be distorted), then this is a sign of a stroke.
- D: the patient’s movements become asymmetrical - he cannot raise both arms or bend his legs simultaneously, one limb lags behind or does not obey at all. Also, a person with a stroke often loses his balance and falls to the ground.
- A: the patient’s articulation (the ability to pronounce words) is difficult, the tongue slurs like a drunk, sometimes he is unable to pronounce the simplest phrase, confuses syllables, stutters or mumbles.
- R: a decision must be made immediately - if at least one of the signs listed above occurs, you must call an ambulance and call a resuscitation team. The minutes count down.
Hemihypesthesia - what is it?
What is hemihypesthesia?
Image source: en.ppt-online.org Hemihypesthesia is a decrease in any type of sensitivity, up to partial or complete loss (anesthesia) on one side of the body (hemianesthesia), usually the opposite side of the brain (BM).
In the case of a stroke, it manifests itself in the form of an acute disruption of the blood supply to the area of the brain responsible for sensitivity or nerve pathways
Hemihypesthesia, as a syndrome, in medicine and neurology, in particular, has other synonyms. It is also called a decrease in sensitivity according to the hemitype (left or right).
Consequences of strokes
One in three people who have a stroke die due to severe brain damage or delays in receiving medical care. The consequences of an attack for those who survive depend on several factors. The most significant of them are the amount of damage to the nervous system, the part of the brain in which the stroke occurred, the timeliness and quality of treatment.
For example, if the brain stem center, which is responsible for vital functions - breathing, heartbeat, thermoregulation and others, is left without oxygen, then the patient’s life will hang by a thread.
In some other situations, the functions of the affected areas are taken over by other nerve centers, making it possible over time to compensate for all violations and return to a full life.
Is full recovery possible after a stroke?
Despite the scientific progress of recent decades, there are still many blind spots in medicine. And first of all, this applies to neurophysiology. Experienced doctors who treat patients after strokes avoid making accurate predictions: in world practice, there are many cases where patients with signs of severe brain damage completely restored their health. At the same time, alas, the opposite stories are not uncommon - when a seemingly insignificant disorder of nervous functions turns into a disability, and even expensive medications and procedures do not have a pronounced effect on the patient’s condition.
Nevertheless, doctors note that the discipline of patients and their relatives, as well as an optimistic attitude, make it possible to achieve tangible results in recovery after a stroke - regardless of the diagnosis and statistics. The desire to gain independence and restore lost functions, be it the ability to speak, strength and sensitivity in the legs and arms, vision, a firm gait without crutches or a cane, sometimes works wonders. But it is also extremely desirable to provide the patient with the necessary organizational and medical support aimed at preventing recurrent attacks and preventing possible complications and injuries. Thus, it is important that rehabilitation takes place in a comfortable and friendly environment, and that relatives or medical workers monitor compliance with medical prescriptions, attend procedures, and supervise the performance of physical exercises.
Doctors assign a significant role in recovery after a stroke to psychological support for the patient: often people who have survived an attack feel depressed due to the loss of their usual abilities.
This is observed in both elderly and young patients, and relatives are not always able to properly support the person, returning him interest in life and motivation to overcome the disease. An experienced psychologist will not only be able to find the right words, but will also suggest effective practical ways to overcome depression.
Forecast for recovery
Most often, older people experience a stroke. It is they who have a complication in the form of paralysis of the arms. In most cases, complete recovery occurs. But this is provided that the patient complies with the recommendations of the attending physician and the rules of rehabilitation.
It takes 6 months, sometimes 1 year, to recover a hand after a stroke . But after a second attack, it is not always possible to cure complications such as paralysis, numbness or loss of sensation. Therefore, many patients remain disabled.
To prevent all these complications, it is necessary to promptly seek help from a doctor. He will make an accurate diagnosis and prescribe treatment, especially if disorders develop at the initial stage.
How long does it take to recover from a stroke?
Experts agree that early initiation of rehabilitation activities, which should last from several weeks to a year, is optimal. Most of the reversibly lost functions, as a rule, return to the patient during the first months after the attack; after the first six months, the progress of recovery slows down significantly, but does not stop. There are cases where certain skills - for example, speech, hearing or sensitivity of paralyzed limbs - returned to the patient several years after the stroke. To increase the chances of such an outcome, it is necessary to continue health procedures even after the end of rehabilitation, as well as from time to time undergo courses of maintenance therapy.
General rules of treatment
A favorable outcome for a disease such as acute stroke depends directly on the time of initiation of qualified medical care.
In the acute period, stroke treatment is carried out in a hospital, the strategic goals are:
- restoration of blood flow through the thrombosed artery;
- minimizing the risk of developing early neurological complications - cerebral edema,
- convulsive syndrome;
- improvement of functional indicators;
- reducing the risk of fatal complications from the heart and blood vessels - death from coronary artery disease and other cardiovascular diseases.
Before hospitalization in the ambulance, measures to reduce intracranial pressure should already begin, regardless of the type of stroke. These include elevated head position, oxygen therapy, and hemodynamic control.
Widely used methods of neuroprotection, such as intravenous drips of magnesium (magnesium sulfate) and sublingual administration of the drug Glycine, have not proven effective. An ambulance must transport a patient with a suspected stroke to a hospital that has CT scanning capabilities. After hospitalization, in the first hours the patient should be in intensive care.
How to treat a stroke in the acute period? The general principles of intensive care for all types of stroke are:
- blood pressure monitoring - maintaining this indicator 10% higher than the numbers to which the patient was adapted before the stroke in order to establish blood supply to the brain in conditions of edema;
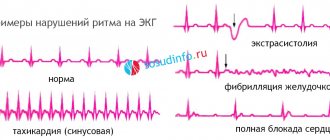
- heart rhythm monitoring - if disturbances are detected, antiarrhythmic drugs are prescribed, as well as drugs to improve the pumping function of the left ventricle and myocardial nutrition;
- control of metabolic indicators in the body - normalization of body temperature, maintaining normal blood sugar levels, water and electrolyte balance, oxygenation, etc.;
- reduction of swelling of the brain substance;
- symptomatic therapy is carried out when appropriate symptoms occur - anticonvulsants, painkillers, antibiotics, connection to a ventilator, etc.; prevention and treatment of possible complications - for example, pneumonia, pulmonary embolism, phlebothrombosis, stress stomach ulcers, etc.
Ischemic stroke
In this situation, conservative methods of treating stroke are used. All patients, within 4-4.5 hours from the moment the first signs of cerebral infarction appear, undergo thrombolytic intravenous therapy to dissolve the blood clot that has blocked the cerebral vessel. This is done to eliminate the cause of the disease and prevent recurrent thrombosis.
The main drug is tissue plasminogen activator (actilyse), a protein that converts the precursor of the enzyme plasmin into its active form, which has a fibrinolytic effect (dissolves blood clots). When started early, this method can quickly alleviate the patient’s condition (motor, speech disorders, etc. decrease).
Treatment of ischemic stroke with thrombolytic drugs is carried out only with the consent of the patient or his relatives with the exact time of onset of neurological symptoms and a confirmed diagnosis on CT. Contraindications are the patient's serious condition and lack of consciousness.
Another method is the prescription of antiplatelet drugs, which reduce the formation of blood clots by inhibiting platelet aggregation. This is not an alternative to thrombolysis, but a necessary measure if it is impossible to carry out it or an addition to it (carried out a day or more after administration of the plasminogen activator).
For treatment after a stroke that occurred no later than 48 hours ago, Acetylsalicylic acid is used in a daily dose of 100 to 325 mg, Dipyridamole MB 200 mg twice a day or Clopidogrel once a day in a dose of 75 mg. Subsequently, Aspirin is prescribed for long-term oral administration (6-9 months), especially to patients with angina pectoris who have undergone stenting or myocardial infarction. Patients with a high risk of venous thrombosis and pulmonary embolism (obesity, diabetes mellitus, long-term bed rest), and cardiac arrhythmias are indicated for subcutaneous administration of heparin drugs followed by a transition to oral anticoagulants (warfarin, Xarelto).
Surgical methods for cerebral infarction are used less frequently; one of them is the installation of a stent to restore lumen in the vessels of the neck or head.
Hemorrhagic stroke
For hemorrhagic strokes, various neurosurgical interventions are very often used. Before the operation, a CT scan of the brain, an angiographic study, and an ultrasound scan are required. With a hemorrhagic stroke, hemorrhages, especially deep ones, can lead to blood breaking into the ventricles and the development of occlusive hydrocephalus (dropsy of the brain), which will require bypass surgery.
Surgery for strokes is carried out for the following purposes:
- remove as much as possible all existing blood clots with minimal damage to the brain substance;
- reduce intracranial pressure at the local and general level;
- restore liquor dynamics.
Contraindications for surgery are the patient's advanced age (over 75 years), lack of consciousness (coma), and the presence of severe concomitant diseases (decompensated diabetes, renal failure, purulent-septic conditions, oncology).
One of the main problems arising with this type of stroke is pronounced vasospasm in the area of hemorrhage. This can further impair blood supply, increase brain swelling and increase intracranial pressure. Antispasmodics are used to relieve spastic phenomena. During the first 24 hours, the patient is prescribed drugs to increase blood clotting in order to prevent repeated hemorrhages or increased bleeding.
Rehabilitation methods
Post-stroke rehabilitation is divided into four main areas:
- Restoration of the motor system . Includes a variety of techniques aimed at combating paralysis. This includes massage, kinesiotherapy, physical therapy, walking rehabilitation, physiotherapy and occupational therapy - restoring skills needed in everyday life.
- Restoration of speech and memory . Within the framework of this direction, a speech therapist (with a specialization in aphasiology) works with the patient, who, with the help of special exercises, returns the patient’s ability to speak clearly.
- Restoration of pelvic functions . Since some patients experience urinary incontinence and problems with stool after a stroke, the rehabilitation doctor prescribes medications and physiotherapeutic procedures to partially or completely restore the functioning of the genitourinary system and intestines.
- Psychological recovery involves consultations with a psychologist, as well as activities aimed at socializing the patient. It is important for people who have suffered a stroke, especially in old age, not to be alone, to communicate with others, and to have a hobby. Therefore, treatment courses in rehabilitation centers often include a cultural and leisure program.
Rehabilitation in acute and early recovery periods of stroke
It is carried out in a hospital setting. At this time, all activities are aimed at saving lives. When the threat to life passes, measures to restore functions begin. Positional treatment, massage, passive exercises and breathing exercises begin from the first days of a stroke, and the time for the start of active recovery measures (active exercises, transition to a vertical position, standing up, static loads) is individual and depends on the nature and degree of circulatory disorders in the brain, from the presence of concomitant diseases. Exercises are performed only on patients who are clearly conscious and in satisfactory condition. For small hemorrhages, small and medium-sized heart attacks - on average from 5-7 days of stroke, for extensive hemorrhages and heart attacks - on 7-14 days.
In the acute and early recovery periods, the main rehabilitation measures are the prescription of medications, kinesitherapy, and massage.
Medications
In its pure form, the use of drugs cannot be classified as rehabilitation, because it is more of a treatment. However, drug therapy creates the background that ensures the most effective recovery and stimulates the disinhibition of temporarily inactivated brain cells. Medicines are prescribed strictly by a doctor.
Kinesiotherapy
In the acute period, it is carried out in the form of therapeutic exercises. Kinesitherapy is based on positional treatment, passive and active movements, and breathing exercises. On the basis of active movements, carried out relatively later, learning to walk and self-care is built. When performing gymnastics, the patient must not be overtired; efforts must be strictly measured and the load gradually increased. Treatment with position and passive exercises for uncomplicated ischemic stroke begin on the 2-4th day of illness, for hemorrhagic stroke - on the 6-8th day.
Treatment by position. Purpose: to give paralyzed (paretic) limbs the correct position while the patient lies in bed. Make sure that your arms and legs do not remain in one position for a long time.
Laying in a supine position. The paralyzed arm is placed under a pillow so that the entire arm, including the shoulder joint, is at the same level in a horizontal plane. Then the arm is abducted to the side to an angle of 900 (if the patient has pain, then they start with a smaller angle of abduction, gradually increasing it to 900), straightened and turned outward. The hand with the fingers extended and spread apart is fixed with a splint, and the forearm with a bag of sand. The leg on the side of paralysis (paresis) is bent in a log at an angle of 15-200 (place a bolster under the knee), the foot is in dorsiflexion at an angle of 900 and is held in this position by resting on the headboard or using a special case in which it is placed foot and lower leg.
Laying in the position on the healthy side is carried out by giving the paralyzed limbs a flexion position. The arm is bent at the shoulder joint and elbow, placed on a pillow, the leg is bent at the hip, knee and ankle joints, placed on another pillow. If muscle tone has not yet increased, the position on the back and healthy side is changed every 1.5-2 hours. In cases of early and pronounced increase in tone, treatment in the supine position lasts 1.5-2 hours, and on the healthy side - 30-50 minutes.
There are other styling options. J.Vantieghem et al recommend alternating the patient's position on the back, on the healthy side and on the paralyzed side.
Laying on the back: the patient's head lies on a pillow, there is no need to bend the neck, the shoulders are supported by the pillow. The paralyzed arm lies on a pillow at a short distance from the body, straightened at the elbow and wrist joints, fingers straightened. The thigh of the paralyzed leg is extended and placed on a pillow.
Positioning on the paralyzed side: the head should be in a comfortable position, the torso should be slightly turned and supported by pillows behind and in front. The position of the paralyzed arm: it rests completely on the bedside table, at the shoulder joint it is bent by 900 and rotated outward, at the elbow and wrist joints it is extended as much as possible, the fingers are also extended and spread apart. Position of the paralyzed leg: the hip is extended, the knee is slightly flexed. The healthy arm rests on the body or on a pillow. The healthy leg lies on a pillow, slightly bent at the knee and hip joints (step position).
Laying on the healthy side: the head should lie in a position comfortable for the patient in line with the torso, slightly turned forward. The paralyzed arm lies on a pillow, bent at the shoulder joint at an angle of 900 and extended forward. Position of the paralyzed leg: slightly bent at the hip and knee, lower leg and foot placed on a pillow. The healthy arm is placed in a position comfortable for the patient. The healthy leg is extended at the knee and hip joints.
When treating with position, it is important that on the side of paralysis the entire arm and its shoulder joint are located at the same level in a horizontal plane - this is necessary to prevent stretching of the shoulder joint bursa under the influence of gravity of the arm.
Passive movements improve blood flow in paralyzed limbs, can help reduce muscle tone, and also stimulate active movements. Passive movements begin with the large joints of the arms and legs, gradually moving to the small ones. Passive movements are performed slowly (a fast pace can increase muscle tone), smoothly, without sudden movements, on both the sick and healthy side. To do this, the methodologist (the person who performs rehabilitation measures) clasps the limb above the joint with one hand, and with the other below the joint, then making movements in this joint to the fullest extent possible. The number of repetitions of each exercise is 5-10 times. Passive movements are combined with breathing exercises and teaching the patient to actively relax muscles. When performing passive movements in the shoulder joint, there is a high risk of injury to the periarticular tissues, so there is no need to perform sharp abduction and flexion of the paralyzed arm at the shoulder joint, or sharp movement of the arm behind the head. To prevent stretching of the shoulder joint bursa, the technique of “screwing” the head of the humerus into the glenoid cavity is used: the methodologist fixes the shoulder joint with one hand, with the other hand clasps the patient’s arm bent at the elbow joint and makes circular movements, pressing towards the shoulder joint.
Among the passive exercises, it is necessary to highlight a passive imitation of walking, which serves to prepare the patient for real walking: the methodologist, clasping the lower third of the shins of both legs, bent at the knee joints, alternately flexes and extends them at the knee and hip joints with simultaneous sliding of the feet along the bed.
When performing passive movements, it is important to suppress synkinesis (cooperative movements) in paralyzed limbs. When performing exercises on the leg in order to prevent synkinesis in a paretic arm, the patient is told to clasp his fingers in the “lock” position and clasp his elbows with his palms. To prevent concomitant movements in the leg when performing movements with the arms, the leg on the side of the paresis can be fixed with a splint.
Following the passive movements with which therapeutic gymnastics begins, they move on to performing active ones.
Active gymnastics, in the absence of contraindications, begins in case of ischemic stroke after 7-10 days, in case of hemorrhagic stroke - after 15-20 days from the onset of the disease. The main requirement is strict dosing of the load and gradually increasing it. The load is dosed by amplitude, tempo and number of repetitions of exercises, and the degree of physical stress. There are static exercises, accompanied by tonic muscle tension, and dynamic exercises: during them the movements themselves are performed. With severe paresis, active exercises begin with those of a static nature, since they are easier. These exercises involve holding your arms and legs in their given position. The table shows exercises of a static nature.
Exercises of a dynamic nature are performed primarily for muscles whose tone usually does not increase: for the abductor muscles of the shoulder, supinators, extensors of the forearm, hand and fingers, abductors of the thigh, flexors of the leg and foot. With severe paresis, they begin with ideomotor exercises (the patient first mentally imagines the movement, then tries to perform it, while pronouncing the actions performed) and with movements in facilitated conditions. Facilitated conditions imply the elimination in various ways of gravity and friction, which make it difficult to perform movements. To do this, active movements are performed in a horizontal plane on a smooth slippery surface, systems of blocks and hammocks are used, as well as the help of a methodologist who supports the limb segments below and above the working joint.
Towards the end of the acute period, the nature of active movements becomes more complex, the pace and number of repetitions gradually but noticeably increase, and exercises for the torso begin (light turns, bends to the sides, flexion and extension).
Starting from 8-10 days (ischemic stroke) and from 3-4 weeks (hemorrhagic stroke), if the patient feels well and is in satisfactory condition, they begin to teach sitting. Initially, he is helped 1-2 times a day for 3-5 minutes to take a semi-sitting position with a seating angle of about 300. Over the course of several days, while monitoring the pulse, both the angle and the sitting time are increased. When changing body position, the pulse should not increase by more than 20 beats per minute; if pronounced palpitations occur, then reduce the landing angle and duration of the exercise. Usually, after 3-6 days, the elevation angle is increased to 900, and the procedure time is up to 15 minutes, then they begin learning to sit with their legs down (the paretic arm is fixed with a scarf to prevent stretching of the joint capsule of the shoulder joint). When sitting, the healthy leg is placed on the paretic leg from time to time - this is how the patient is taught to distribute body weight on the paretic side.
Next, they begin to learn to stand next to the bed on both legs and alternately on the paretic and healthy leg (the knee joint on the affected side is fixed using the hands of a methodologist or a splint), walking in place, then walking around the room and corridor with the help of a methodologist, and with improving gait - using a three-legged crutch or stick. It is important to develop in the patient the correct walking stereotype, which consists of friendly flexion of the leg at the hip, knee and ankle joints. For this purpose, footprints are used, and to train “triple bending of the leg” on the side of the paresis, wooden planks 5-15 cm high are installed between the footprints. The last stage of learning to walk is training to walk on stairs. When walking, the patient's paretic arm must be secured with a scarf.
The rehabilitation measures carried out should bring the maximum possible restorative effect. The most gentle care techniques are shown in the table below.
Along with teaching the patient to walk, exercises are carried out to restore everyday skills: dressing, eating, and performing personal hygiene procedures. Exercises and techniques for restoring self-service are reflected in the table below.
Massage
Massage begins for uncomplicated ischemic stroke on days 2-4 of illness, for hemorrhagic stroke - on days 6-8. The massage is carried out when the patient lies on his back and on his healthy side, daily, starting from 10 minutes and gradually increasing the duration of the massage to 20 minutes. Remember: vigorous tissue irritation, as well as a fast pace of massage movements, can increase muscle spasticity! When selectively increasing muscle tone, massage should be selective.
On muscles with increased tone, only continuous planar and grasping stroking is used. When massaging opposing muscles (antagonist muscles), stroking is used (deep planar, tong-like and intermittent grasping), gentle transverse, longitudinal and spiral rubbing, light shallow longitudinal, transverse and tong-like kneading.
Direction of massage: shoulder-scapular girdle → shoulder → forearm → hand; pelvic girdle → thigh → lower leg → foot. Particular attention is paid to massage the pectoralis major muscle, in which the tone is usually increased (slow stroking is used), and the deltoid muscle, in which the tone is usually reduced (stimulating methods in the form of kneading, rubbing and tapping at a faster pace). Massage course 30-40 sessions.
In a hospital setting, rehabilitation measures are carried out no longer than 1.5-2 months. If it is necessary to continue rehabilitation treatment, the patient is transferred to an outpatient rehabilitation facility.