Pregnant women and their families usually expect one answer from an ultrasound examination - what is the sex of the child. For an obstetrician-gynecologist, a research method is necessary to promptly identify impaired blood flow during pregnancy and abnormal fetal development.
The management plan and delivery tactics depend on this. To understand the mechanisms of the disorder, it is necessary to consider the capabilities of the circulatory system between mother and child.
Structure of the uteroplacental blood flow
Mother and child are connected not only by the placenta, but also by a complex system of blood vessels. Therefore, all joint blood circulation is usually divided into levels that cannot exist in isolation, but work only in combination.
- The central part of the system is the placenta. It ensures the “absorption” of products from the maternal blood through the villi that have grown deep into the wall of the uterus. At the same time, the blood of mother and child does not mix. Several rows of special cells form a hematoplacental barrier, which is a serious obstacle to substances unnecessary for the fetus. Through it, the waste blood returns to the mother's venous system.
- The second part of the blood flow consists of the branches of the uterine arteries. If before pregnancy in the female body they are in a collapsed state and are called spiral, then from the period of 1 month they lose the muscle layer that can cause spasm. And by four months, the arteries transform into full-fledged trunks, filled with blood and heading to the placenta area. It is this mechanism, useful for feeding the fetus, that can turn out to be fatal during uterine bleeding: the walls of the vessels can no longer contract.
- The vessels in the umbilical cord form the third pathway of blood flow. There are 2 arteries and a vein here. They connect the baby with the placenta and form the fetal-placental circle. Reduced blood flow at this level causes the most severe damage to the fetus.
Types of disturbances in blood flow through the uteroplacental system
A change in blood circulation in the woman-child mechanism is not such a rare complication during pregnancy and is the cause of gestosis in pregnant women, as well as premature birth. There are primary and secondary placental insufficiency.
Primary
A primary disorder of blood flow through the uteroplacental system develops in the early stages of pregnancy up to 16 weeks. The causes of this pathology during this gestational period are disturbances in the processes of placentation and implantation.
At periods up to 16 weeks, an acute form of blood flow disturbance usually develops, accompanied by detachment of the baby's place (placenta).
Secondary
The secondary development of hemodynamic imbalance of the vascular bed during gestation develops under the influence of external factors that affect the fetus, the pregnant woman and the already formed placenta. As a result of a secondary disturbance of placental blood circulation, a chronic disturbance develops. More often it occurs in the 4th month of pregnancy.
Depending on the severity, secondary blood flow disorders can be divided into:
- decompensated (the fetus experiences growth retardation);
- compensated (changes are regulated by the mother’s body, as a result of which the child’s development is not disrupted);
- subcompensated (the fetus stops growing and developing normally, the risk of intrauterine loss of the baby increases);
- critical (quite rare, leads to gestational loss).
How is placental circulation disrupted?
Poor blood flow associated with the placenta is called placental insufficiency. It can occur at any stage of pregnancy in two forms.
Acute appears suddenly, even during childbirth, and does not depend on the duration of pregnancy. The fetus falls into a state of hypoxia (oxygen deficiency), which threatens its death.
The main pathological mechanisms of this condition:
- premature placental abruption;
- heart attack due to thrombosis.
Chronic often complicates the course of pregnancy after 13 weeks. Symptoms appear in the third trimester. The mechanism of formation is early aging of the placenta due to the deposition of fibrin on the villi.
As a result of changes in the structure of chorionic villi (placental tissue), the functioning of the hematoplacental barrier ceases, metabolic processes between the maternal body and the fetus are disrupted
Negative consequences in such conditions, depending on the degree of violation, can lead to inevitable death of the fetus.
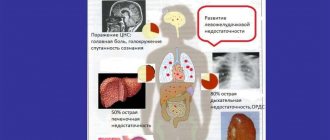
How dangerous is NMPC for the fetus?
Fetal hypoxia is one of the main consequences of NMPK
Reduced blood supply to the fetus can cause the following obstetric complications:
- Reduced weight and size (intrauterine growth retardation syndrome);
- Heartbeat disturbances, in addition to tachycardia (rapid rhythm) and bradycardia (slow rhythm), arrhythmia can also develop as a result of disturbances in the electrolyte composition of the blood;
- Violation of the acid-base balance in the fetus’s body (change in blood pH);
- Pathological functioning of the child’s hormonal system;
- A pronounced decrease in fat depots, which is also manifested by low fetal body weight;
- Threat of miscarriage;
- A critical disruption of blood flow can cause intrauterine fetal death.
Causes of blood flow disorders during pregnancy
Various reasons can cause disruption of uteroplacental blood flow. These include common maternal diseases:
- pathology of the neuroendocrine system (diabetes mellitus, diseases of the thyroid gland and adrenal glands, changes in the hypothalamus region of the brain stem);
- lung diseases (emphysema, bronchial asthma);
- disorders in the cardiovascular system caused by developmental defects, the consequences of hypertension, a tendency to hypotension;
- renal pathology (chronic nephritis, pyelonephritis, especially in the stage of renal failure;
- anemia (anemia) associated with deficiency of iron and vitamins;
- conditions accompanied by increased blood clotting contribute to increased thrombus formation in the vessels of the placenta;
- acute and exacerbation of chronic infectious processes cause corresponding inflammation in the placenta, vascular edema and reduction in blood flow; in the first trimester this can result in miscarriage.
Pathology of the uterus creates local conditions for inadequate blood flow:
- any changes in the layers of the uterus (myometrium, endometrium);
- malformations (for example, “bicornuate”, “saddle-shaped” uterus);
- underdevelopment (hypoplasia);
- tumor formations from muscle tissue (fibroids), especially in a primiparous woman over the age of 35; at a younger age, small fibroids help compensate for blood flow.
The causes of insufficient blood flow include unfavorable conditions during pregnancy in the following cases:
- multiple births;
- Rhesus conflict;
- preeclampsia;
- breech presentation of the fetus;
- pathological placenta previa.
The risk of impaired blood flow occurs when:
- previous abortions;
- maternal smoking, alcoholism and drug addiction;
- constant nervous environment associated with social or everyday unsettlement;
- violation of proper nutrition of a woman.
Reasons that can lead to disruption of blood flow in the mother-placenta-fetus system
- Anemia in a pregnant woman. A decrease in hemoglobin levels leads to an acceleration of blood flow in all vessels, including the uterine arteries. This happens for one simple reason: with anemia, the body tries to increase the delivery of oxygen to the tissues by increasing the speed of circulating blood. This is a compensatory reaction. The same thing happens in the uteroplacental system.
- The pathology of placental attachment (low placentation, previa) is characterized by reduced blood flow, since in the area of the lower segment of the uterus the muscle layer is much thinner than in other areas. A similar situation develops when the placenta is attached to the area of the uterine scar (usually after a previous cesarean section). The thinned area of the scar cannot fully provide blood flow, so the amount of blood that flows to the fetus may be insufficient for the normal functioning of the developing organism.
- Preeclampsia (late toxicosis) is one of the most common causes of impaired blood supply to the uteroplacental system, since this obstetric complication causes damage to small vessels.
- Various infectious diseases suffered during pregnancy. Some microorganisms infect the placenta and cause pathological changes in its tissue, which can cause placental insufficiency.
- Immune-conflict pregnancy (according to the Rh system, blood groups, etc.) in severe cases is accompanied by the development of hemolytic disease of the fetus. With this pathology, anemia develops in the baby, and as a result, fetal blood flow is disrupted.
- Unstable blood pressure in a woman affects the speed of blood in the vessels, as well as the volume of blood flow in the uteroplacental system.
- Malformations of the uterus. Pronounced changes in blood flow occur with such an anomaly as a bicornuate uterus. In this case, there is a septum in the uterine cavity that divides it into two parts: equal or unequal (in the presence of a rudimentary horn). Thus, pregnancy develops in one of the uterine cavities. At first glance, it can be assumed that the obstacles to the development of pregnancy lie precisely in the mechanical factor (the reduced size of the uterine cavity cannot create conditions for the normal development of the fetus). But it is not so. After all, hidden reserves for stretching muscle tissue are enough for full gestation. The main reason that creates a real threat is the disruption of adequate blood supply to the fetus. Normally, the two uterine arteries are the main source of arterial blood for the fetus. In addition, during pregnancy they begin to actively expand in diameter, and a large number of connecting vessels (anastomoses) appear between them, which ensures normal blood flow. In a bicornuate uterus, such processes do not occur, the uterine arteries are not connected to each other, the arterial network does not expand, which means that the proper amount of blood does not reach the placenta.
- Pathology of umbilical cord vessels. Sometimes during the study it is possible to identify a change in the number of vessels (for example, a single umbilical cord artery), which can become a serious cause of impaired blood flow to the fetus.
- Pathological processes at the level of the endometrium (inner lining of the uterus) can also cause disruption of blood flow. This is usually preceded by various inflammatory diseases (endometritis), surgical procedures (multiple abortions, diagnostic curettages) or bad habits (smoking, drinking alcohol).
- Uterine fibroids. As you know, during pregnancy myomatous nodes grow, and accordingly their blood supply increases. Thus, “robbing” the fetal blood flow occurs. A direct correlation has been revealed: the larger the size of the nodes, the more pronounced the insufficiency of uteroplacental blood flow, since part of the blood is lost to nourish the fibroids.
- Multiple pregnancies are often accompanied by impaired blood supply. Firstly, this pregnancy requires the development of several fetuses, which means that the placental site is significantly increased in size compared to a singleton pregnancy. In addition, sometimes there is a shunting (transition) of most of the blood flow to one of the fetuses to the detriment of the other, which is called “feto-fetal transfusion syndrome”. The fetus, whose blood supply is reduced, acts as a donor. As a rule, its mass is reduced and it is smaller in size. The other fetus, on the contrary, acts as a recipient because its blood flow is increased. It is larger in size. However, you should not think that the recipient fetus is in a more “winning” situation, because the baby’s heart is not yet adapted to increased blood flow. Therefore, this fetus is also at high risk of complications. In other words, with feto-fetal transfusion syndrome, the blood flow of both fetuses is impaired.
- Diabetes mellitus in the mother leads to damage to the inner wall of the arteries. The disease often debuts during pregnancy.
Types of chronic placental insufficiency
Depending on the development of consequences for the fetus and the ability of the mother’s body to adapt, 4 forms or stages of chronic placental insufficiency are distinguished:
You can also read: When does fetal heartbeat appear?
- compensation - the mother’s body fully protects the fetus by improving blood flow through other pathways, and the child does not feel a lack of oxygen, develops normally, is born on time and develops well;
- subcompensation - the mother is not able to fully compensate for the lack of nutrition, and the fetus lags behind in development, there is a risk of complications and congenital defects;
- decompensation - accompanied by a complete disruption of the adaptation mechanisms, normal pregnancy is impossible, the fetus develops serious defects that are incompatible with viability, and death in utero is very likely;
- critical - due to severe changes in the structure of the placenta, further gestation of the fetus is impossible, inevitable death occurs, any treatment is ineffective.
Types of fetoplacental insufficiency
First of all, placental insufficiency is classified into chronic and acute forms. Acute pathology can occur at any stage and even during delivery. Meanwhile, in the placental tissues, gas exchange is disrupted, leading to acute fetal hypoxia or the death of the baby. Often this phenomenon occurs against the background of premature placental infarction or detachment, bleeding or blood clots.
Chronic forms of fetoplacental insufficiency are diagnosed much more often and occur mainly during the second trimester of gestation, although they are detected only in the third trimester. On the surface of the villi, which grow into the uterine wall, fibrin begins to be deposited, which interferes with the normal course of metabolic processes. As a result, premature placental aging begins.
Chronic insufficiency of fetoplacental blood supply is divided into the following types:
- Critical. With this form, serious functional and morphological changes develop in the structures of the placenta, which cannot be influenced in any way, so fetal death becomes inevitable.
- Subcompensated deficiency. With such a violation, the female body cannot cope with disturbances in placental activity, so fetal development is delayed, which leads to complications during gestation and fetal development.
- Decompensated - when compensation mechanisms lose the ability to deal with pathological placental changes, therefore the norm of indicators during the development of pregnancy is violated, the fetus begins to suffer from hypoxia, cardiac dysfunction, developmental delays, etc. The likelihood of intrauterine fetal death is high.
- Compensated deficiency is considered the most favorable of all of the above, since the fetus continues to develop without suffering from various abnormalities. With such a deficiency, the female body is able to adapt and compensate for the deviations that have occurred to the child. If a woman receives the correct treatment, then such deviations will not affect the health of the baby and the timing of delivery.
What degrees of blood flow disturbance does placental insufficiency cause?
A comparison of clinical manifestations and ultrasound examination results made it possible to distinguish 3 degrees of blood flow disturbance between mother and fetus.
The first is characterized by minimal changes at the uteroplacental level, provides a “reserve” of time of about a month for treatment and full recovery without consequences, there are 2 types:
- Ia - only the uteroplacental blood flow is reduced, with the fetal-placental blood flow unchanged. It manifests itself as a delay in fetal development in 90% of cases.
- Ib - fetal-placental circulation suffers, but the uteroplacental circulation remains normal. Delayed formation and development of the fetus suffers somewhat less (in 80% of cases).
The conclusion is issued after examining all components of the fetal blood flow
The second is that the disorder occurs both at the level of the uterine and umbilical vessels; hypoxia can be fatal to the fetus.
Third, blood circulation indicators are at a critical level, and it is even possible that the direction of blood flow is reversed (reverse).
For clinicians, such a classification provides an opportunity to accurately determine the level of disorders and choose the most appropriate treatment tactics.
Blood supply system between mother and baby
During gestation, a close connection is established between the child and the mother, which is also called the fetoplacental system. It consists of several departments.
- The central role is given to the placenta, which grows into the uterine wall with villi and through them nourishes the fetus in the uterus with the necessary substances. Moreover, maternal and fetal blood do not mix, since there is a hematoplacental barrier through which the blood is filtered, returning back to the woman.
- The arterial network of the uterine body is also part of the fetoplacental system. Before conception, these arteries are spasmodic and twisted in the form of a spiral, but already from the first month of pregnancy, the muscle layer that provides the spasmodic state resolves, and by the fourth month of gestation, the arteries are transformed into special trunks that carry blood to the placental structures, fully participating in the blood supply. This phenomenon was specifically provided by nature for better intrauterine nutrition of the child. If uterine bleeding begins, the vascular walls will no longer be able to contract, which can lead to heavy blood loss, even death.
- Another part of the blood supply system between mother and fetus are the umbilical vessels, which form another route of blood supply. A vein and two arterial canals pass through the umbilical cord, which connect the fetus to the placenta. If blood flow disturbances occur in this part, the fetus is subject to severe damage.
Symptoms of impaired blood flow
If the impaired blood flow is compensated, then the woman does not feel any abnormalities, but learns about them only after the examination.
Pronounced manifestations occur in acute form and chronic decompensation:
- the motor activity of the fetus increases sharply or completely disappears (at 28 weeks, normal development is accompanied by ten movements per day), this symptom requires immediate contact with an obstetrician-gynecologist;
- a slow increase in abdominal circumference, detected during monthly examination and measurement in the antenatal clinic (associated with excessive formation or lack of amniotic fluid);
- late toxicosis;
- high blood pressure;
- large weight gain;
- swelling in the legs;
- the appearance of protein in the urine.
The most dangerous thing is bleeding from the vagina. This sign can be regarded as beginning placental abruption. You must not delay in providing medical care.
Diagnosis of disorders
If the development of placental blood flow disorders is suspected, the patient undergoes a comprehensive examination. The leading role in diagnosis is given to Doppler ultrasound in combination with ultrasound examination. Such techniques make it possible to promptly identify pathological blood flow disorders and determine the degree of complications caused by them. Typically, Doppler testing is prescribed for premature placental aging, insufficiency or excess amniotic fluid, congenital genetic pathologies or fetal defects, hypoxic manifestations or intrauterine growth retardation.
Diagnostics
The most complete picture of blood circulation between the uterus and the fetus is obtained through Doppler ultrasound, which is performed on all women three times during pregnancy.
The technique allows:
- measure blood flow by the speed of movement of the formed elements;
- determine its direction in arteries and veins;
- record changes before clinical manifestations.
The effect is based on the properties of ultrasonic wave reflection and is completely safe for the child and mother.
All changes are recorded on the monitor, measured with special sensors, and can be photographed in the required format.
By comparison with normal indicators, a conclusion is made about the degree of pathology. Violations can be detected at any level, in the vessels:
- umbilical cord,
- uterus,
- fetus
The doctor has time to prescribe treatment and check it at the next examination.
A type of Doppler ultrasound is Doppler ultrasound. It is prescribed for:
- maternal concomitant pathology;
- suspected premature aging and disruption of the placental barrier;
- signs of high or low water;
- preliminary data on intrauterine growth retardation, the formation of congenital malformations of the fetus;
- presence of genetic diseases in the family;
- clinical symptoms of fetal hypoxia.
The examination can reveal:
- thinning of the placenta;
- increase in growth area;
- intrauterine infection.
The method of long-term inpatient monitoring of the degree of fetal hypoxia allows you to see the results of using medications
Diagnostic methods
The “gold standard” for blood flow disorders in the mother-placenta-fetus system at the moment in obstetrics is a Doppler study. This method opens up the possibility of recognizing even the most minor changes, as it is highly sensitive and informative.
Doppler is a type of ultrasound examination that is based on the use of the Doppler effect. The essence of the study is to measure the frequency of ultrasonic waves reflected from moving objects. When studying blood vessels, the moving particles are the formed elements of blood, in particular, red blood cells, as the most numerous cells. Registration of the obtained data and comparison with the norm is called Dopplerography.
What are the benefits of Doppler ultrasound?
- Modern ultrasound machines make it possible to examine the direction and speed of blood flow in the uterine arteries, umbilical cord vessels, and even intraplacental blood flow.
- Thanks to color mapping, it is possible to separately examine blood flow in vessels with different directions of blood (arteries and veins). The direction of arterial blood on the device is reflected in red, and venous blood in blue.
- It has been proven that the use of this method during pregnancy does not have a negative effect on the development of the fetus.
- A unique feature of the method is to predict the development of pregnancy. What does this mean? Many studies have shown that disturbances in the blood flow of the uteroplacental system appear a little earlier than any clinical manifestations of fetal suffering (decreased body weight, change in heart rhythm, etc.). This means that with timely diagnosis of fetal blood supply disorders, the doctor has a small amount of time to make the right decision. An example of this is the detection of a change in blood flow, which is called a “dicrotic notch,” in 90% of cases before the development of clinical manifestations of gestosis (edema, increased blood pressure, the appearance of protein in the urine). Doppler sonography is widely used in obstetric practice, as it gives doctors the opportunity not only to promptly recognize blood flow disturbances, but also to even prevent the development of certain pregnancy complications.
Recently, the results of the use of Doppler sonography not only during pregnancy, but also during childbirth are increasingly being published. Conducted studies prove that the effectiveness of contractions can be assessed by measuring the diastolic blood flow velocity in the uterine arteries. Thus, this research method can even predict weakness or impaired coordination of labor at the beginning of the first stage of labor.
Case from practice
An unusual situation that occurred in the maternity ward forced obstetricians and gynecologists to think about the use of Doppler ultrasound during childbirth.
A 25-year-old woman without any concomitant pathology was admitted into labor. home with regular contractions every 3-5 minutes. First birth, urgent.
According to the anamnesis: the pregnancy proceeded without complications, no fetal pathology was detected, all ultrasound protocols with Doppler measurements were within normal limits.
The first stage of labor proceeded physiologically; when the cervix was fully dilated, the woman in labor was transferred to the delivery room.
However, during pushing, seemingly inexplicable phenomena began to occur: the fetal heartbeat was restored during pushing, but in the intervals between pushing it slowed down significantly. Although, as a rule, everything happens the other way around. In this regard, it was decided to perform an ultrasound to study blood flow in the vessels during childbirth. The result of the study surprised everyone: during the intervals between contractions, the fetus pressed the umbilical cord with its hand, as a result of which the blood flow was significantly disrupted. As hypoxia increased in the child’s body, his arms weakened and he let go of the umbilical cord, meanwhile the blood flow was restored. Taking into account the obtained picture, it was decided to speed up the management of the second stage of labor using auxiliary aids. Thus, thanks to Doppler measurements, doctors managed to avoid serious complications.
Secondary diagnostic methods
In addition to Doppler sonography, there are other research methods that indirectly indicate a violation of blood flow:
- Collection of complaints. If blood circulation is impaired, the fetus experiences hypoxia, which is manifested by an increase in the baby’s physical activity. Typically, pregnant women complain of active fetal movement.
- Listening to the heartbeat with a stethoscope can also help in diagnosis. Slowing or accelerating the rhythm beyond the physiological norm may also indicate hypoxia.
- CTG recording. Registration of CTG for 40-60 minutes may be sufficient to diagnose signs of intrauterine fetal hypoxia.
- Some ultrasound indicators (premature aging of the placenta, study of the biophysical profile) can document the unfavorable condition of the fetus.
Important! A slight decrease in estimated fetal weight on ultrasound does not necessarily indicate developmental delay and blood flow disturbances. An isolated measurement of fetal weight is not very informative, since this indicator is also largely influenced by genetic factors. Therefore, it is necessary to take into account the anthropometric indicators of the parents (height, weight) and their birth weight. Only a combination of decreased fetal weight and impaired blood flow during Doppler ultrasound provides grounds for a diagnosis of “intrauterine growth retardation syndrome.”
Treatment of pathology
The possibility of maintaining pregnancy with the help of conservative treatment remains with the degree of impaired blood flow Ia and b. The second degree is considered borderline, the third requires urgent surgical delivery.
Treatment takes into account the pathogenesis of disorders. To achieve results it is necessary to influence all links:
- In case of mild disturbance of microcirculation, Chofitol (with a mineral-herbal composition) is prescribed, in more severe cases - Actovegin, Petoxifilin.
- If a mother’s tendency to form blood clots and disrupt the aggregation properties of blood is detected, then drugs such as Curantil, Trental are indicated. They can improve blood flow through the vessels.
- If low blood pressure is detected, Venofundin, Stabizol, ReoHES are used.
- Vasodilators - No-spa, Eufillin in injections - eliminate spastic contraction of blood vessels.
- It is recommended to reduce the tone of the uterus with the help of Magnesia, the drug Magne B6, this acts as an antihypoxic way to improve blood flow.
- A group of vitamins with antioxidant action eliminates negative consequences (vitamin E, ascorbic acid).
Medications are prescribed by a doctor. If necessary, the woman is offered hospitalization. This allows:
- provide bed rest;
- Constantly monitor the progress of pregnancy.
If there is an effect of conservative treatment, the woman independently carries to term and gives birth to a child. If there are no results, doctors may decide to perform an early cesarean section. In the third stage, only surgical delivery is indicated.
Doppler
This unusual name has a diagnostic procedure that identifies any pathologies of blood flow in arteries and veins. As a result, a Dopplerogram is constructed using specialized equipment, which displays the frequency difference between the sent and reflected signal. The study is carried out in standard mode or with color mapping, that is, the movement of blood through the arteries is displayed in color. The latter option allows you to quickly and accurately detect even mild disturbances in uteroplacental blood flow.
Doppler measurements are performed while lying on your back or side. In this case, a more truthful result may be obtained on the side, since tone begins on the back of many pregnant women, provoking various pathologies. The specialist covers the area under study with gel and begins to move the sensor over it.
This study is prescribed to all pregnant women along with the first (18-22 weeks) and second (32-34 weeks) screening. It can also be carried out at intermediate stages if indicated.
What to do to prevent blood flow disorders?
Gynecologists urge women at risk to prepare themselves for pregnancy in advance and prevent unplanned conception.
Choosing the right body position while sleeping helps fetal blood flow
If you are already pregnant, it is recommended:
- avoid emotional and physical overload;
- eliminate bad habits;
- organize nutritious meals for the pregnant woman;
- monitor daily walks and stay in a ventilated room;
- do special gymnastics for pregnant women, yoga exercises;
- control body weight, carry out monthly weighing and measurement of abdominal circumference;
- It is considered more beneficial to sleep on the left side; this position reduces pressure on the inferior vena cava, which runs to the right of the uterus, but in some cases, with stagnation in the kidneys, sleeping on the right side improves the outflow from these important organs.
Modern diagnostic methods and approaches to the management of pregnant women make it possible to prevent severe disorders. However, many possibilities depend on the woman herself and her desire to have a healthy heir.
What emergency situations might develop?
Pathological changes that accompany blood flow disturbances during gestation can lead to dangerous situations that pose risks to the lives of both the woman and the fetus and require drastic measures to be taken to stabilize the condition of both.
- acute lack of oxygen in the unborn baby (hypoxia);
- premature aging of the placenta;
- detachment of the baby's place (placenta);
- the appearance of developmental defects in the baby;
- gestational loss.
In most cases, in such situations, the baby is removed urgently, by performing a cesarean section.
Therapy
If the fetus does not receive enough blood, it will develop hypoxia. When such a condition is detected, gynecologists must respond immediately and offer the girl the most appropriate treatment regimen, which will be based on simultaneous action on several stages of pathogenesis.
Initially, medications are selected that have the ability to improve the process of blood microcirculation, for example, it could be Actovegin or Pentoxifylline. Particular attention is paid to maintaining good blood flow in the vessels and stabilizing blood pressure.
For this purpose, medications based on hydroxyethyl starch are prescribed, including: Stabizol, Infucol, Voluven, ReoHES, Venofundin. These drugs act as an osmotic solution of starches, due to which the liquid does not leave the lumen of the blood vessels. It is best to take them during gestosis, since this way you can avoid the occurrence of edema and stabilize blood flow.
To relieve arterial spasm, medications with a vasodilating effect are prescribed. Eufillin, No-shpa or Magnesia are often prescribed (the drugs are best used in injection form). Hypoxia can also be prevented or eliminated by eliminating uterine tone. To do this, a woman will have to take Magnesia, Ginipral or vitamin B6.
It is not enough to eliminate hypoxia, it is also necessary to prevent the likelihood of complications, so Tocopherol, Ascorbic acid and Chophytol are introduced into the therapeutic complex. Some patients are injected intravenously with a 5% concentration of glucose solution, which makes it possible to remove toxins from the body.
To improve the condition of the placenta and saturate it with phospholipids, Essentiale is prescribed. To improve cellular nutrition, Cocarboxylase is prescribed, and if pregnancy occurs in a woman who has a history of uterine fibroids, taking Curantil will be useful.
When carrying a child, a woman must be prescribed a study of uteroplacental blood flow using Doppler ultrasound. As medical practice shows, it is this diagnostic method that makes it possible to identify all deviations, even minor ones; accordingly, doctors have the opportunity to start therapy in a timely manner and stabilize the condition of the pregnant woman.
Methods to improve blood flow in the uterus
There are several methods for solving the issue of blood circulation in the uterine cavity. Let's look at each of them in more detail.
Gynecological massage
There is an opinion that thanks to the procedure it is possible to normalize blood circulation in the uterus without using medications, eliminate unpleasant symptoms, and also significantly improve the condition of the reproductive system organs.
The procedure is contraindicated during menstruation, at the stage of undergoing therapy against infectious and inflammatory diseases of the reproductive organs, as well as after childbirth, artificial termination of pregnancy and miscarriages.
Progressive doctors consider these barbaric methods, accompanied by serious side effects, and do not recommend these procedures at all.
Physiotherapy
The doctor may prescribe the following types of physiotherapy:
- Magnetotherapy. One of the most effective methods, which also allows you to stimulate the outflow of fluid, while providing a countercurrent effect.
- Ultrasound procedure. Allows you to improve blood flow in the tissues of the uterus, normalize the functioning of the appendages and adjust hormonal levels.
- Phototherapy. Among other things, this procedure enhances the bactericidal effect of medications used in treatment.
- Electrotherapy. Through this procedure, it is possible not only to improve blood circulation in the uterine tissues, but also to relieve muscle spasms.
Physical activity
You can also improve blood circulation in the tissues of the uterus by performing certain exercises:
- bike;
- squats;
- stand on all fours;
- tension in the buttocks when lying on your back;
- exercises with fitball.
Drug treatment
A more radical method of improving blood circulation in the tissues of the uterus is drug therapy. By taking certain medications, which are prescribed individually, you can achieve the following results:
- improve the elasticity of the vascular network inside the uterus;
- speed up blood flow;
- improve vascular permeability;
- reduce the fragility of the capillary network;
- strengthen the walls of large veins and arteries.
Among the main medications prescribed by the doctor:
- Troxevasin;
- Troxerutin;
- Phlebodia 600.
Treatment methods for different degrees of pathology
The first degree of the disease involves taking medications that improve blood circulation. Doctors will also conduct Doppler measurements and cardiotocography (heartbeat) of the fetus in dynamics. Research should be carried out 1-2 times every 7 days. If the dynamics are positive, the woman will continue to carry the baby until it is born. If the indicators worsen, it is necessary to conduct daily examinations to prevent irreversible changes and perform an emergency caesarean section in time. With normal fetal development, childbirth can occur naturally.
Stage 2 blood flow disorders during pregnancy can also be treated. Usually the same drugs are used as in the first case, but the woman will be offered hospitalization. Doctors will monitor changes in the body and, if necessary, carry out early delivery.
The third degree cannot be treated in any way, since irreversible consequences begin to appear. In this case, specialists do not risk the child’s life and prescribe an emergency operation.