Causes of vascular dementia
The pathology occurs as a result of acute or chronic ischemic damage to the cerebral cortex and individual subcortical nuclei. This causes the death of neurons responsible for human cognitive abilities (cognitive functions).
Important! If other areas of the brain are damaged, paralysis, hearing or vision impairment, disorders of the vestibular apparatus, and pathologies of the respiratory organs may occur, but the patient’s intelligence remains at the same level.
Experts identify the following causes of vascular dementia:
- Ischemic stroke;
- Development of repeated embolization against the background of cardiac pathologies (endocarditis, atrial fibrillation);
- Vasculitis of various origins (autoimmune, infectious);
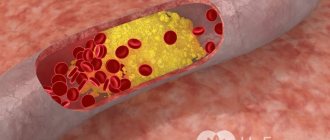
- Chronic cerebral ischemia due to arterial hypertension, atherosclerosis, hypotension;
- Nonspecific vasculopathy.
The main reason for the development of vascular dementia at a young age is bad habits: alcoholism, smoking and drug addiction. However, it should be remembered that the rate of development of dementia can be influenced by the following provoking factors:
- Advanced age;
- History of diabetes mellitus;
- Heart pathologies (coronary disease, defects, fibrillation);
- Brain injuries;
- Various oncopathologies;
- Hypertension or hypotension;
- Autoimmune vascular pathologies of a systemic nature;
- Dyslipidemia;
- Male gender;
- Genetic predisposition.
Important! Some experts attribute the low educational level of the patient to the provoking factors of vascular dementia. A highly educated person indicates greater brain reserves, and therefore delays the development of cognitive disorders.
Causes
Dementia of the vascular type develops as a result of the death of brain cells caused by a circulatory disorder (lack of or complete stoppage) in any part of it. Disruption of blood flow to brain tissue can occur acutely or be chronic.
Acute circulatory disorder
Acute vascular dementia develops with ischemic or hemorrhagic stroke. Ischemic stroke can be triggered by pathologies such as atherosclerosis, some heart diseases and cerebral vascular abnormalities. In this case, the cerebral arteries are blocked by a thrombus or embolus, which impedes blood flow.
Hemorrhagic stroke is accompanied by hemorrhage that occurs when pressure increases and pathologies of the walls of brain vessels (due to atherosclerosis, intoxication or inflammation). Blood pours into the brain tissue by breaking the integrity of the vessel or “leaks” through the wall of the affected artery.
Both types of stroke are acute, with pronounced symptoms and lead to the immediate death of a large number of brain cells, which entails the development of dementia. The severity of the disorders depends on the location and size of the lesion.
Chronic circulatory pathologies
Chronic circulatory disorders are not accompanied by pronounced manifestations. In this case, brain neurons die gradually due to impaired blood flow in small vessels (with atherosclerosis) or poor circulation, characteristic of cardiovascular failure. Due to compensation mechanisms for such pathologies, vascular dementia in the initial stages goes unnoticed for a long time by the patient and his loved ones.
At-risk groups
Patients with pathologies such as diabetes mellitus, arterial hypertension, vascular diseases of the brain, heart and peripheral circulatory system have a higher risk of developing vascular dementia. The greatest likelihood of being affected by the disease was found in people over 60 years of age and smoking patients. It is also known that men suffer from vascular dementia much more often.
Mechanism of disease development
Acute disturbances in cerebral blood flow or chronic insufficiency of blood supply to the brain lead to the fact that some neurons stop receiving oxygen and nutrients. This causes cell death.
If the lesion leads to infarction of a small number of neurons, then other brain cells are able to compensate for the loss. In such cases, only damage to a large area of the brain leads to the development of symptoms of vascular dementia. However, if neurons that perform cognitive functions are affected, then the death of even a small group provokes the onset of dementia.
Symptoms at each stage
The first symptoms of vascular dementia begin with a noticeable expression of conservatism in the patient’s views, judgments and actions. At the same time, some character traits are aggravated. Excessive distrust or obstinacy, frugality and other changes appear.
Mental activity and memory gradually deteriorate. This is soon accompanied by trembling of the limbs and blurred speech.
In addition, vascular dementia, which appears as a result of damage to certain areas of the brain, is manifested by a variety of symptoms:
- The death of cells in the midbrain is characterized by confusion and darkness. With the further development of the disease, the patient withdraws into himself, loses interest in what is happening around him, in communicating with loved ones. He doesn't care about his appearance and stops taking care of it.
- Damage to the cells of the hippocampus (parts of the brain in the temple area), which is responsible for long-term storage of information, leads to memory impairment, including amnesia. The patient cannot remember events that happened today or recently, although he can reproduce those that happened a long time ago.
- The death of neurons in the frontal lobes of the brain manifests itself in indifference, apathy, laziness, and loss of interest in communication. There may be illogical behavior, which is expressed in the monotonous repetition of a phrase or word that has long been known to the patient.
- With the death of nerve cells in the subcortical regions, the patient’s attention is significantly distracted, which makes it impossible to concentrate on one task or object. He cannot highlight the main thing and determine the secondary in the information received, or analyze it. All his endeavors are unsuccessful.
In addition to cognitive impairment, almost all patients have problems with urination, which often becomes spontaneous. Emotional disorders and instability during the course of the disease often lead to depression, loss of optimism and self-confidence.
Stages of the disease
In the pathogenesis of dementia, it is customary to distinguish 3 stages, which are characterized by different symptoms:
- Light form . This stage is characterized by vague symptoms that patients do not notice. Relatives and people close to you may suspect the development of dementia. Usually there is a slight decrease in intellectual activity and a sharp change in mood. However, the patient is able to control his emotions and his actions, he solves everyday problems on his own and does not need help.
- Moderate form . The development of more pronounced symptoms is characteristic: the inability to independently navigate in space, memory loss, personality disorder, which leads to behavioral deviations. This makes life significantly more difficult for patients. Many patients become aggressive. At this stage, patients need help from others in everyday activities.
- Severe form . The patient needs constant help and supervision from loved ones or medical personnel. At this stage there is a deep breakdown of the psyche. The patient is unable to eat and perform hygiene procedures independently, and cannot control urination and defecation. Patients do not recognize their relatives.
Clinical picture
A characteristic feature of the disease is the development of neurological syndromes in the patient against the background of cognitive disorders. After a stroke, cognitive impairment is observed within 1-2 months from the onset of the disease. In case of chronic disturbance of cerebral blood flow, the period can take up to 6 months.
The severity and nature of cognitive impairment is determined by the area of brain damage. However, the following typical symptoms of vascular dementia are distinguished:
- Memory loss. The symptom develops in the initial stages of dementia. Patients usually forget some things from the past;
- Impaired ability to assimilate new material (movements and words). However, passive recognition persists in the initial stages;
- Speech disorder. At first, patients forget some words, but subsequently patients are unable to understand the meaning of speech. Gradually a person loses the ability to count, write and read;
- Inability to self-care: patients are unable to dress, perform hygiene procedures, cook and eat food;
- Slowness and rigidity of thinking;
- Difficulties with purposeful switching and maintaining attention;
- Disorientation in space and time;
- Emotional incontinence, leading to violent crying, irritability, aggressiveness. This condition can cause depression and psychosis.
Read more about the symptoms of dementia in our article.
See also:
- Kidney failure in old age
- Ischemic cerebral stroke: symptoms, prognosis, treatment
- Low blood pressure in older people
Patients also develop neurological disorders, which can be pronounced or almost invisible. Many patients note changes in gait and frequent falls, the development of paresis, impaired control over the functioning of the pelvic organs, and the occurrence of epileptoid seizures.
Important! Dementia of the vascular type is characterized by a wave-like course - the listed symptoms can progress, then stabilize. In rare cases, short-term restoration of function is possible.
Signs of pathology
Dementia in older people does not have one set of symptoms, as each person who develops dementia may behave differently. However, it is possible to identify some signs that will be the same for everyone. Most often, the patient experiences the following symptoms:
- Gait disturbance (lameness, body instability when walking, etc.).
- The appearance of epileptic seizures.
Neurologist Dmitry Nikolaevich Shubin tells how to recognize an epileptic seizure and how to help the patient:
- Urinary dysfunction.
- Deterioration of attention, memory and other cognitive impairment.
- Impairment of physical functions.
Also, symptoms depend on the stage of development of the pathology.
initial stage
It is difficult to identify manifestations of vascular dementia at this stage, since such symptoms can be characteristic of many diseases. Among them:
- The appearance of apathy, irritability or other neurosis-like disorders.
- Emotional instability and frequent mood swings.
- Depressive state.
Psychiatrist Mikhail Aleksandrovich Tetyushkin talks about the signs and treatment of depression:
- Inattention.
- Disorientation in space on the street or in an unfamiliar room.
- Sleep disorders (frequent nightmares, insomnia, etc.).
Middle stage
Now the symptoms are becoming clearer, and doctors can use them to diagnose vascular dementia:
- Sudden mood swings, when apathy suddenly changes into aggressive behavior.
- Memory lapses are still only short-term.
- Disturbance in home orientation.
This may be useful: What is cerebral ischemia in a newborn?
- Vestibular dysfunction or other physical disorders.
- Difficulty in communication. A person may forget the names of objects, be unable to carry on a conversation, etc.
Severe stage
At this stage, all the symptoms of vascular dementia become pronounced:
- A person cannot navigate in space.
- The occurrence of hallucinations or delusions.
- The appearance of aggression for no reason.
- Memory losses. The patient cannot say what happened a minute ago, does not recognize loved ones, etc.
- Difficulty moving or even being unable to get out of bed.
- The patient needs round-the-clock supervision by loved ones.
There are signs that are highly likely to indicate the development of pathology:
- Slight recovery of cognitive performance. Doctors have not yet been able to figure out what this might be connected with. Usually, this is preceded by mental stress. In this case, the patient’s condition may return to normal levels, but the pathology itself does not disappear and after a while, vascular dementia will begin to manifest itself again.
- A gradual development that often precludes diagnosis. In most cases, relatives admit that they noticed some changes in the patient, but they focused attention on this only when irreparable changes had occurred. After a stroke, vascular dementia develops only in 20-35% of cases.
- Surgical operations or treatment with coronary artery bypass surgery can precede the development of dementia.
Diagnostic measures
With timely diagnosis of vascular dementia, a complete recovery of the patient is possible. In other cases, a correct diagnosis can reduce the rate of development of pathology. For this purpose, the following diagnostic measures are used in modern neurology:
- Examination of the patient, careful collection of medical history;
- Psychological testing to determine the presence and severity of disorders;
- Pressure monitoring;
- Determination of glucose and cholesterol in the bloodstream to determine the presence of diabetes mellitus and atherosclerosis;
- Radioisotope research;
- Carrying out magnetic resonance or computed tomography. The techniques allow us to determine the degree of damage to brain tissue;
- Dopplerography of cerebral vessels allows you to study blood flow in the brain;
- Angiography is radiography of brain vessels.
An accurate diagnosis can only be made on the basis of a comprehensive diagnosis and comparison of the results obtained.
How to distinguish vascular dementia from Alzheimer's disease
MRI or CT is used as diagnostics; without these studies, it is very difficult to obtain data about the disease and determine its type only by the symptoms that appear. Experts focus on the following indicators:
- If memory and cognitive impairment are observed after a stroke, a diagnosis of vascular dementia is made.
- With signs of Alzheimer's syndrome, the pathological process develops slowly but steadily; with vascular dementia, symptoms arise suddenly, sharply, with a gradual course, and sometimes fluctuations in the manifestation of symptoms occur.
- Often with vascular dementia, signs of focal brain damage, weakness of the limbs (hemiparesis), impaired reflexes of the right and left arms and legs, and the severity of the Babinski reflex appear.
- Gait disturbance (shuffling, slowness, unsteadiness) is also a symptom of vascular dementia. Patients often complain of dizziness, confusing it with instability.
- In chronic ischemia, a characteristic symptom of vascular dementia is incontinence. This symptom is observed in almost all patients.
It is noteworthy that one patient may exhibit both symptoms of vascular dementia and signs of Alzheimer's syndrome. Modern scientists have been able to conduct research that has shown that deformation of cerebral vessels becomes the main factor in the development of Alzheimer's syndrome and one of the main reasons for the onset of the neurodegenetic process. In this regard, many forms of dementia are mixed in nature - vascular-degenerative.
We recommend
“Products for people with dementia that will make life more comfortable and safer” Read more
Features of dementia therapy
Treatment measures should be aimed at eliminating the pathological factors that caused vascular dementia and correcting cognitive impairment. Medicines are prescribed on an individual basis, based on the clinical picture of the disease and the severity of pathological processes, the presence of concomitant pathologies.
General treatment tactics include the following:
- Therapeutic gymnastics, which involves regularly performing simple physical exercises for the legs and arms;
- Dietary nutrition, which involves excluding spicy, fatty and fried foods, dairy products from the diet;
- Vasodilators that are classified as ACE inhibitors (Lisiropril, Perindopril). This allows you to normalize blood pressure in hypertension;
- Statitis (Atorvastatin, Simvastatin, Lovastatin). The drugs help normalize cholesterol levels in the bloodstream;
- Periodic use of diuretics to prevent the development of a hypertensive crisis;
- Antiplatelet drugs (Aspirin, Clopidogrel). This helps prevent the development of repeated disturbances in cerebral blood flow, as well as myocardial infarction;
- Light sedatives based on valerian, motherwort. In some cases, the prescription of anticonvulsants is required;
- Preparations based on Gingko Biloba (Tanakan, Memoplant). Medicines can improve cognitive function;
- Antioxidants (Mexidol, Cytoflavin, Omega-3). Taking medications of this group allows you to protect nerve cells from the negative effects of free radicals;
- Nootropics (Piracetam, Nootropil, Phenotropil, Lucetam). The drugs are used to improve brain nutrition and restore cognitive functions;
- Neuroprotectors (Actovegin, Cortexin, Ceraxon). Medicines help preserve the functionality of healthy neurons.
Along with drug treatment, patient care and maintaining the patient’s psychological comfort play an important role. Many people with vascular dementia require constant care from relatives. Patients also need to regularly solve puzzles, crosswords, and puzzles. Regular walks in the fresh air and water procedures can improve the well-being of patients.
Cognitive impairment and dementia of vascular origin
The subject of active research in recent years is the development of a holistic concept of cognitive impairment and vascular dementia. Vascular dementia can develop in various forms of both acute and chronic cerebrovascular pathology, mainly of an ischemic and hypoxic nature [1]. In the early stages of chronic cerebrovascular insufficiency
patients often complain of decreased memory (“forgetfulness”), absent-mindedness, concentration disorders and instability of active attention. Most often, memory for names, numbers, and recently occurring events decreases. The ability to memorize new material decreases, it becomes more difficult to retain what has been read, what is planned for implementation is forgotten, and the need to write it down arises. It becomes difficult for patients to comprehend a large amount of information, which leads to a certain decrease in performance and limitation of creative possibilities in people engaged in mental work. At the same time, professional memory and memory of past events are preserved. This applies more to RAM than to logical memory. Often, a decrease in memory and performance is regarded by others as a result of overwork, and not as a manifestation of cerebral vascular insufficiency. During neuropsychological research, the preservation of the level of generalization, the correspondence of judgments to the general educational and cultural level, and the preservation of the stock of ideas and skills are noted. Decreased memory for current events in patients with vertebrobasilar insufficiency is associated with chronic ischemia of the medial parts of the temporal lobes, primarily the hippocampus and mammillary bodies. With vertebrobasilar insufficiency, attacks of transient global ischemia are also observed, during which working memory (the ability to remember new information) is impaired for several hours. The patient looks absent-minded, he is disoriented in space and time, sometimes excited, persistently tries to find out from those around him where he is, how he got here, but being unable to remember the answers, he constantly asks the same questions. With the return of the ability to remember, orientation is also restored, only the episode itself is amnesic. Vascular dementia is diagnosed based on a combination of the following signs (ICD-10): - dementia; — heterogeneity of impairments of cognitive functions (some of which can be significantly impaired while others are relatively intact); - focal neurological symptoms (paresis, asymmetry of tendon reflexes, pyramidal signs, pseudobulbar syndrome, disturbances of statics, coordination, sensitivity, pelvic organ function); - anamnestic, clinical and neuroimaging data (leukoaraiosis, multiple medium and small cerebral infarctions), which are symptoms of vascular disease.
The clinical manifestations of vascular
dementia
are varied. In 45% of cases, dementia occurs after a stroke (post-stroke dementia), in 30% of patients it increases in waves in the absence of obvious clinical signs of cerebrovascular accident (CVA) (non-stroke type of course), in 25% of cases dementia appears and progresses both during stroke and and in the non-stroke type of the disease. Vascular dementia is characterized by a progressive deterioration of cognitive functions, a decrease in memory for past and current events, a slowdown in mental processes, a decrease in mental activity and the level of judgment, a store of information and knowledge, a violation of chronological dating and time orientation while maintaining criticism, awareness of one’s own inadequacy and basic personal attitudes. . The ability to memorize new material is, as a rule, more significantly impaired than memory for distant events. Vascular dementia rarely reaches the level of deep complete collapse of the psyche, characteristic, for example, of the final stage of Alzheimer's disease. Vascular dementia is characterized by both long periods of decompensation or, on the contrary, stabilization and even reverse development of mnestic-intellectual disorders, as well as short-term changes in the state of mnestic-intellectual functions, therefore the degree of severity of this type of dementia often fluctuates quite significantly in one direction or another.
Diagnostics
Clinical diagnosis of vascular dementia is associated with certain difficulties, since its manifestations are nonspecific. Therefore, it is necessary, especially in a progressive, non-stroke course, for differential diagnosis with other forms of dementia, primarily with Alzheimer's disease. The basis for diagnosing vascular dementia can be the criteria presented in the one developed by V. Hachinski et al. (1975) “ischemic scale”, which includes 13 points - a list of clinical signs of the disease, each of which is assessed in points. Of greatest importance are the acute onset of dementia, stepwise progression and variable course, data on arterial hypertension (AH) and a history of stroke, and the identification of focal neurological symptoms. Vascular dementia is also characterized by relative preservation of personality, manifestations of general atherosclerosis and atherosclerosis of the arteries supplying the brain. In vascular dementia, coronary heart disease, atrial fibrillation, and heart failure are often observed. According to the ischemic scale, vascular dementia is diagnosed with a score of 7 or more, while Alzheimer's disease is diagnosed with a score of 4 or less. In recent years, the diagnostic value of the “ischemic scale” has been confirmed by numerous studies. When used correctly, the accuracy of clinical diagnosis of dementia of vascular origin reaches 70%. However, a number of studies have shown that some of the main features listed in this scale are not mandatory. For example, such an important symptom as a history of stroke occurs in 88% of patients with cortical and only 71% of patients with subcortical vascular dementia. In addition, with progressive vascular leukoencephalopathy (PSLE), as a rule, there is a non-stroke course, and cognitive impairment increases gradually. The use of the “ischemic scale” allows, despite its obvious shortcomings (non-stroke forms of dementia are not taken into account, which primarily applies to PSLE), to carry out rapid diagnosis of the main forms of dementia, and is invariably included in the original or modified version (for example, with the addition of CT data or MRI) to the list of scales in the study of various forms of late-life dementia. Neurological examination helps identify a number of symptoms that often accompany vascular dementia. These include asymmetric pyramidal insufficiency, postural instability, gait changes such as frontal dysbasia, pelvic disorders, and visual field defects. Urination and gait disturbances are considered clinical markers of vascular dementia. They are believed to be caused by bilateral changes in the frontal descending pathways. With vascular dementia, dysarthria, violent laughter and crying, and reflexes of oral automatism, characteristic of pseudobulbar syndrome, are often encountered. Fluctuations in the severity of cognitive impairment with step-like progression and alternating periods of stabilization and regression, intermittent states of nighttime confusion and daytime “clearance” are also characteristic of vascular dementia. The subtypes
of vascular dementia include (ICD-10): - dementia with acute onset;
- multi-infarct dementia; — subcortical dementia; - mixed cortical-subcortical dementia. There are some features of psychopathological and neurological symptoms that are more characteristic of certain forms of vascular dementia. Acute-onset dementia
occurs within 1 month.
(but not more than 3 months) after a stroke. It may be caused by single infarctions or hematomas located in functionally significant areas of the brain (angular gyrus, frontal, parietal, temporal lobes, thalamus, cerebellum). Dementia does not increase and even decreases over time. The degree of its regression varies and depends on the location of the infarction or hematoma, their location in the dominant or subdominant hemisphere, unilateral or bilateral changes, and previous changes in the brain, which were asymptomatic before the stroke. Among the forms of dementia caused by the occurrence of single infarctions, particular importance is attached to “thalamic” dementia, which develops with infarctions in the region of the median and anterior nuclei of the thalamus. The disconnection of the fibers connecting the thalamus and reticular formation with the frontal and limbic lobes of the brain leads to a symptom complex reminiscent of “frontal syndrome”, which is characterized by aspontaneity, adynamia, hypersomnia, disorientation, decreased memory and attention, slowdown of all mental processes, uncriticality, inadequacy, emotional disturbances. The most pronounced cognitive impairment is observed with infarctions in both thalami. Associated focal neurological symptoms are usually mild. Moderate paresis, hyperkinesis, and oculomotor disturbances are rarely observed. In most cases, in the acute period of stroke, urinary control is impaired. Great importance in the development of cognitive impairment is attached to infarctions localized in the cerebellar hemisphere
opposite the dominant cerebral hemisphere.
The disconnection of the connections of the cerebellum with the frontal, parietal, temporal and occipital lobes is manifested by a decrease in attention, memory, difficulty in assimilating new information, difficulty constructing a speech utterance, impairment of abstract thinking, counting, and spatial organization of mental activity. In some cases, with cerebellar infarction, mutism is observed, which in the acute period of a stroke is mistakenly interpreted as dementia. A characteristic feature of cognitive impairment in these cases is its recovery over time. Multi-infarct dementia
is characterized by a decrease in cognitive functions caused by multiple medium and small infarcts localized in the cortex, white matter of the cerebral hemispheres, basal ganglia, thalamus, basilar part of the pons, and cerebellum.
Dementia in these cases develops acutely or increases in steps, and the main reasons for its development are considered to be the destruction of a significant volume of brain tissue in the corresponding brain regions and the disconnection of their connections with other brain structures. Dementia was most often detected in cases in which the number of medium and small heart attacks was more than 10. Cognitive impairment manifests itself in the form of a gradual decline in memory, impairment of counting, writing, spatial orientation, and praxis. Subcortical vascular dementia,
caused by the occurrence of hypertensive small deep infarcts (MDI) in the white matter of the cerebral hemispheres and leukoaraiosis, is recognized on the basis of a history of stroke-like episodes.
If at the early stage of the disease changes in mental status are minimal, then at a later stage a picture of the so-called apathetic dementia of the subcortical type is formed in combination with pseudobulbar manifestations. In MHI, mental traits characteristic of changes in this localization predominate predominantly in the frontal region. This type of vascular dementia is characterized by its combination with bilateral pyramidal symptoms, most often in the legs. Dysarthria, monoparesis, isolated hemiparesis, walking disorders (gait with frequent small steps and relatively widely spaced legs - “marche a petit pas”), urinary incontinence, forced crying and laughter may be detected. Cognitive, emotional disturbances, gait disorders and pelvic organ function disorders in PSLE are associated with changes in the white matter of the frontal lobes, where frontothalamic, fronto-limbic and other fibers pass from the centers that control the automaticity of walking and from the centers that control pelvic functions. Clinically, PSLE is difficult to distinguish from dementia caused by multiple small superficial infarcts (MSI) and MHI of the brain, especially since these forms of vascular pathology often coexist. However, PSLE is characterized by a longer course, as well as the existence of periods of stabilization, during which a decrease in intellectual functions does not occur. There are certain differences in the characteristics of cognitive impairment in cortical and subcortical vascular dementia. In subcortical vascular dementia, disturbances in the dynamics of mental functions predominate, manifested by decreased attention, memory, visual-spatial perception, slowness of mental processes, spontaneity, narrowing of the range of interests and apathy. With cortical vascular dementia, along with an early decline in memory and intelligence, individual focal symptoms are observed: visual field impairment, hemiparesis, asymmetry of tendon reflexes, changes in higher cortical functions (elements of aphasia, agraphia, acalculia, apraxia). For cortical dementia, caused by multiple infarcts in areas of adjacent blood supply, a combination of visual disorientation, apraxia, memory impairment and muscle weakness, mainly in the arms, is more typical. A single infarction in the cerebral cortex rarely causes dementia, but several times increases the risk of its development. Cerebral infarction, i.e. its focal necrosis, leads to dementia, as its mass decreases. The location of the infarction also plays an important role. For example, a single infarction in the area of the angular gyrus is accompanied by the occurrence of Gerstmann's syndrome (alexia, agraphia, dyscalculia, aphasia and constructive apraxia), which can mimic dementia. The difference in the nature of cognitive impairment in cortical and subcortical dementia clearly appears when analyzing memory impairment. Cortical dementia is characterized primarily by impairments in memorizing new information. For subcortical dementia, a “defect in memory traces” is more typical, therefore, with subcortical dementia, patients can recognize or remember, at a prompt, previously presented material (words, images), which they are not able to actively reproduce. Determining the severity of dementia
is based on assessing the degree of everyday independence: - with mild dementia, the patient only needs outside help to a small extent and is generally able to take care of himself; - with moderate dementia, the patient needs daily, albeit limited, assistance; - with severe dementia, the patient is not able to care for himself and needs constant care. Vascular dementia on CT or MRI is characterized by a combination of cerebral infarctions, leukoaraiosis, moderate expansion of the lateral ventricles and cerebral sulci. Multi-infarct dementia develops with medium infarctions, MPI and MHI (often clinically asymptomatic), which are detected in both the gray and white matter of the cerebral hemispheres, subcortical - MHI predominantly in the white matter, usually in combination with leukoaraiosis. The severity of leukoaraiosis and the degree of dilation of the ventricles of the brain determine the severity of cognitive impairment, but complete correspondence between the neuroimaging picture and the clinic is not always observed. Thus, a moderate decline in cognitive function in patients with chronic cerebrovascular insufficiency usually develops against the background of extensive diffuse changes in the white matter (the volume of which exceeds 10% of the total volume of the white matter of the cerebral hemispheres) or multiple MHI in both hemispheres of the cerebral hemisphere. On the other hand, cognitive impairment is detected when the lateral ventricles dilate and the density of white matter decreases in the region of the anterior horns of the lateral ventricles. When diagnosing vascular dementia, one should also take into account the possibility of post-stroke depression in patients who have suffered a stroke, one of the manifestations of which is impaired cognitive function [2]. Signs of depression such as melancholy, guilt, apathy, anorexia, weight loss, sleep disturbance, tearfulness, and psychomotor retardation may also be detected. Therefore, in clinical practice, in some cases, it is important to distinguish between depression and the formation of vascular dementia, which is carried out by psychiatrists and psychologists using special diagnostic scales. Evidence in favor of depression is: lack of effort when performing neuropsychological tests (frequent answers “I don’t know”), variability in test performance, improvement in test performance when attracting attention, the same degree of memory impairment for recent and distant events. It is important to emphasize that the participation of a psychologist and psychiatrist in the diagnosis of vascular dementia helps to avoid its overdiagnosis, since disorders of cognitive and intellectual-mnestic functions are detected in almost every patient with multiple cerebral infarctions and widespread diffuse changes in the white matter of the cerebral hemispheres. However, even a very thorough psychological and psychiatric examination of these patients makes it possible to diagnose dementia in only some of them. The main differential diagnostic criterion is normalization of neuropsychological status during treatment with antidepressants.
Therapy
Treatment of chronic cerebrovascular accidents is aimed at preventing their progression, improving blood supply to the brain, and correcting individual syndromes and symptoms. The most effective measures in this direction are the elimination or correction of the main risk factors for the development of chronic cerebrovascular accidents, which include hypertension, heart disease, atherosclerosis of the cerebral arteries, disorders of the rheological properties of blood, smoking, diabetes mellitus, obesity, hyperlipidemia, psycho-emotional stress, and alcohol abuse. Treatment methods for chronic cerebrovascular accidents include: antihypertensive therapy, the use of lipid-lowering drugs, improving blood supply to the brain using antithrombotic drugs, neuroprotective therapy, correction of cognitive impairment, asthenic syndrome and depression [1, 3–5]. Considering the polymorphism of the clinical manifestations of chronic musculoskeletal disorders, it should be noted that there is a high risk of polypharmacy, therefore preference is given to drugs with multimodal action. The maximum effect of these drugs was observed in patients with mild and moderate neurological disorders, in the early stages of chronic cerebrovascular accidents [1, 6]. Neuroprotective therapy is aimed at preserving neurons and enhancing their functions. For this purpose, neurometabolic stimulants and drugs with antioxidant effects are used. Over the past two decades, drugs with a cholinergic effect and drugs with an effect on the glutamatergic system have been used to treat patients, initially proposed for the treatment of Alzheimer’s disease, but later showing high effectiveness in chronic cerebrovascular disease [1, 7]. It has been shown that choline alfoscerate penetrates the blood-brain barrier and is metabolized to form two metabolites: choline (a precursor of acetylcholine) and glycerophosphate (a precursor of phosphatidylcholine, which is part of the phospholipids of neuronal membranes), thereby promoting neuroprotection and restoring the structure and function of the synaptic network. The use of Cereton for cognitive disorders of vascular origin is based on the indicated pharmacological properties of choline alfoscerate. Long-term therapy with Cereton (choline alfoscerate) can achieve a significant effect in the form of improvement of cognitive and behavioral functions, reduction of depressive and asthenic disorders. At the beginning of the course of treatment, Cereton can be used IV or IM at a dose of 1000 mg/day for 10–15 days, with further transition to oral administration at the optimal daily dose of 1200 mg (400 mg 3 times/day). The duration of treatment can vary from 3 to 6 months. [1, 7]. Memantine
, a modulator of the glutamatergic system, proved effective in clinical studies of it in vascular dementia and was recommended for use.
The drug had a positive effect on memory and other cognitive functions, as well as on emotional and motor disorders in patients. In addition, an increase in activity levels, improved concentration and an increase in the pace of activity were noted. Memantal is the only generic of memantine that has confirmed therapeutic equivalence to the original drug. Its effectiveness has been demonstrated in Alzheimer's disease [8, 9], including when transferring patients from the original memantine [9, 10]. A promising direction for the treatment of chronic cerebral infarction may be the use of drugs that can be involved in the system of protecting the brain from oxidative stress, reducing the brain's need for oxygen, increasing its resistance to hypoxia and having an antioxidant effect. Most antioxidants have both neuroprotective and nootropic effects. The drug ethylmethylhydroxypyridine succinate,
being a structural analogue of vitamin B6, has in its pharmacological formula a metabolite of the tricarboxylic acid cycle - succinate, which provides an antioxidant and antihypoxic effect.
The Russian company produces this drug under the name Neurox. Thanks to the multifactorial mechanism of action, the pharmacological effects of the drug are realized at three levels: neuronal, vascular and metabolic. The clinical effect of the domestic antioxidant Neuroxa (ethylmethylhydroxypyridine succinate) in patients with chronic urinary tract obstruction is manifested in improved general condition, reduction of headaches, dizziness, improvement of memory and attention [11]. Neurox is prescribed 500 mg intravenously for 2–4 days, then 250 mg intramuscularly for 14 days. In recent years, among neurotrophic drugs that affect the restoration of cognitive functions, a certain place is occupied by the precursor of choline, citicoline [12]. Citicoline (cytidine-5-diphosphocholine) is a natural derivative of nucleotides and is a complex organic molecule that functions as an intermediate in the biosynthesis of cell membrane phospholipids, capable of being involved in brain protection by stabilizing cell membranes and reducing the formation of free radicals. A number of studies have shown the effectiveness of its use in ischemic stroke and chronic cerebral ischemia. Recently, new generic dosage forms have been widely introduced into practice. Among them is the domestic drug Neypilept. The drug is produced from an Italian substance in the form of a solution for intravenous and intramuscular administration (125 and 250 mg/ml), as well as for oral administration in bottles of 30 and 100 ml. The drug confirmed therapeutic equivalence to the original citicoline in the treatment of ischemic stroke in a multicenter comparative study (n=152) [13]. The creation of a universal neuroprotective agent used for cognitive impairment and dementia of vascular origin is unlikely. Therefore, combined but individually oriented long-term neuroprotective therapy and therapeutic cooperation between the patient and the doctor (adherence to treatment) seem to be more promising approaches (Table 1).
In conclusion, it should be emphasized that timely and systematically carried out treatment, together with the rational organization of work and everyday life, can not only prevent the progression of the disease, but also significantly improve the condition of patients.
Prognosis and life expectancy
If the pathology was identified at an early stage, then in 15% of cases it is possible to completely cure dementia. In other cases, the prognosis is unfavorable - the disease ends in death. Life expectancy depends on many factors, so it is difficult to predict.
If the disease develops slowly and the patient retains everyday life skills for a long time, the patient can live up to 20 years from the moment the pathology is discovered. In severe cases, life expectancy rarely exceeds 7-8 years.
Vascular dementia is a pathology that develops against the background of acute or chronic impairment of cerebral blood flow. The disease gradually leads to personality disintegration and loss of cognitive abilities. However, effective therapy, qualified care and constant care for the patient can slow down the course of the disease and prolong the patient’s life.
Treatment
The main goal of therapy is to stabilize the patient's condition. Inpatient treatment is indicated in cases where dementia is accompanied by comorbid (concomitant) disorders. Treatment of moderate vascular dementia is carried out at home - the patient takes medications prescribed by the doctor. The main groups of drugs indicated for vascular dementia:
- Cholinergic (acetylcholinesterase inhibitor - Donepezil, NMDA glutamate receptor blocker - Memantine). They prevent the breakdown of the neurotransmitter acetylcholine, which ensures neuromuscular transmission. Glutamatergic transmission is modeled, providing cortico-cortical and cortico-subcortical connections between neurons. Improve cognitive functions, stimulate daily activity, reduce the appearance of behavioral disorders and apathy.
- Normothymic (Valproic acid). They stabilize mood and regulate biological rhythms.
- Tranquilizers. Eliminate manifestations of anxiety.
- Hypnotics (Zopiclone). Regulate sleep and wakefulness patterns.
To treat vascular dementia in elderly patients, antipsychotics (Chlorprothixene, Sulpiride) are used, which help correct behavioral disorders. In parallel, treatment of vascular pathologies is carried out, and blood pressure, glucose and lipid concentrations in the blood are regularly monitored.
The course of therapy with cholinergic drugs lasts several months or years. Other medications are used until a therapeutic effect is achieved, for example, benzodiazepines (Tofisopam) - until anxiety states are eliminated, Valproic acid - until the psycho-emotional background is stabilized, Zopiclone - for a course of 7-10 days. Along with taking medications, other treatment methods are used, which include psychotherapy and occupational therapy.