The most common consequences of stroke are:
- Sudden fainting.
- Involuntary urination.
- Loss of ability to move independently.
- Impaired ability to recognize individual body parts.
- Frequent dizziness, noises in the head, double images before the eyes.
- Speech dysfunction: confusion, difficulty finding words and pronouncing them.
- Frequent loss of balance, impaired ability to navigate in space.
- Partial dysfunction or complete paralysis of some limbs, part of the body, one of the sides.
- Loss/impairment of vision, hearing, touch, smell, sensitivity of nerve endings.
The majority of patients treated in the neurology department of our clinic are people who have suffered a stroke. During their treatment, doctors solve two strategic problems:
- Secondary prevention of recurrent stroke.
- Treatment (drug, non-drug) and correction of neurological disorders.
Preventing recurrence of attacks
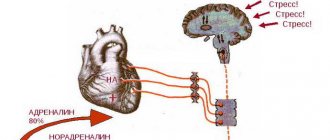
25% of patients who have had an ischemic stroke are at risk of experiencing a recurrence. The greatest likelihood exists within the next year. In this regard, it is important, after taking emergency measures to save the patient, to engage in secondary prevention. Let us note that AI is not an independent disease, but one of the symptoms of disorders in the functioning of the cardiovascular system. This determines the set of preventive measures:
- Drug therapy aimed at eliminating cardiovascular diseases and rapid regression of neurological disorders.
- Lifestyle modification: getting rid of bad habits (smoking, alcohol abuse), correcting body weight (bringing it to normal), performing special physical exercises, following the principles of proper nutrition, including reducing the amount of animal fat consumed.
Emergency medical care call card example hypertension
I 11.9 GB with predominantly cardiac involvement without (congestive) heart failure ( Morbus cordis hypertensivus sine insufficientia cordis):
Ds. Hypertension stage II-III, degrees 1-3, uncomplicated/complicated hypertensive crisis.
I 10 Essential hypertension ( Hypertensio arterialis essentialis (primaria) ):
Ds. Arterial hypertension 1-3 degrees (without hypertension),
Ds. Stage I hypertension.
—————-
Classification
1st degree - 140/90 - 160/100 mm 2nd degree - 160/100 - 180/110 mm 3rd degree - more than 180/110 mm
Stage I - no signs of target organ damage.
Stage II - target organ damage: LV hypertrophy, retinal vasoconstriction, proteinuria, increased. creatinine up to 175 µmol/l. Stage III - heart failure, angina pectoris, MI, stroke, hemorrhages and exudates in the retina, creatinine over 175 µmol/l, aortic dissection, occlusive arterial diseases.
—————-
Hypertension, deterioration (outside of crisis):
Moderate headache, relatively gradual and moderate increase in blood pressure, no more than 20-30 mm Hg. from normal blood pressure. HELP:
ECG. Antihypertensive therapy is not required or only tablet drugs are indicated.
Contraindicated: Short-acting Nifedipine (except pregnant women)
If SBP increases by more than 20 mm: Moxonidine
0.4 mg or
Captopril
12.5-25 mg sublingually.
Tactics.
Hospitalization is not indicated*.
—————- *The need for planned treatment in the cardiology department if treatment in the therapeutic department is ineffective is determined by the head of the cardiology department. in a general manner or at the level of interaction between the heads of both departments (or upon the direction of a local physician and in agreement with the head of the cardiology department). Examination of conscripts with hypertension is carried out in the therapeutic department at the place of residence.
Uncomplicated hypertensive crisis ( crisis hypertensiva sine complicationibus) :
An increase in blood pressure to individually high values (more than 30% of the patient’s usual figures), there are no signs of target organ damage.
Hyperkinetic crisis
(type 1 crisis). Fast development. Duration 2-4 hours. a predominant increase in systolic blood pressure, anxiety, tachycardia, hyperemia (spots) of the skin. In the early stages of the disease.
Hypokinetic crisis
(type 2 crisis). Slow development, often long and severe (up to several days). Diastolic blood pressure is predominantly elevated. Pale skin, predominance of cerebral and cardiac symptoms. In the later stages of the disease with damage to target organs.
Chest pain (cardialgia), often caused by systolic overload of the left ventricle (aching, stabbing pain in the left half of the chest).
There is usually no need for parenteral therapy.
No emergency hospitalization is required.
HELP:
ECG (ECP). Reduce blood pressure by no more than 25% within 3-4 hours.
Recovery process
Stroke is the No. 1 cause of chronic disability in the world. 40% of people unwittingly develop physical and psychological dependence on loved ones, doctors, nurses. However, neurological disorders tend to regress naturally. The main task of specialists is to speed up this process.
The body's ability to recover is based on the mechanism of neuroplasticity:
- Departments of the central nervous system may be reorganized.
- Neurons have the ability to undergo structural and functional changes.
The recovery process has three stages:
- Spicy. Spontaneous recovery.
Immediately after AI (within a week), many body functions resume:
- cerebral edema decreases;
- blood circulation improves in areas bordering the lesion.
- Subacute. Full recovery.
During treatment the following changes occur:
- Brain tissues are functionally reorganized.
- The tissue around the lesion increases its activity.
- Synaptogenesis is activated.
- Chronic. The compensation is improved coordination and increased muscle mass.
Movement restoration
This is the first important task of rehabilitation.
Loss of coordination and loss of mobility occurs in 80-90%, of which only 30% of patients remain able to move independently immediately after an attack. In this area, research is continuously being conducted and methods with a high level of efficiency are being developed. Today, three of them are most often used:
- A method for learning a specific skill. A rehabilitation specialist helps the patient set a specific task and solve it. As a result, the patient develops and learns the most productive movement strategy.
- Forced movement therapy. In this case, the limb that was not damaged at the time of the stroke is deliberately immobilized. As a result, the entire load falls on the injured leg/arm. Daily household activity helps restore the functionality of the organ.
- Bilateral training. In this case, motor tasks are performed simultaneously by both the healthy and the injured limb.
Symptoms
Symptoms of lung cancer
varied:
- cough is the most common and early symptom (often constant, dry, hacking in nature; wet - when inflammation is attached);
- hemoptysis (sputum the color of “raspberry jelly”);
- dyspnea;
- chest pain (of varying intensity). Physical symptoms are characteristic only of late stages of the disease.
- asymmetry of the chest, lag in breathing;
- in the presence of lobe atelectasis - increased vocal tremors, dullness or dullness, harsh breathing, wheezing;
- enlargement of the liver, peripheral lymph nodes (metastases);
- phenomena of exudative pleurisy with hemorrhagic exudate.
Symptoms of the late stage (tumor growth into neighboring tissues and organs):
- swelling of the jugular veins, swelling of the face, neck, upper extremities (“Stokes collar”) - compression of the superior vena cava;
- retraction of the eyeball, constriction of the pupil, drooping eyelid (Horner's syndrome) - compression of the cervical sympathetic nerve;
- symptoms of peptic ulcer of the stomach - infiltration of the vagus nerve;
- hoarseness - compression of the vagus nerve;
- dysphagia - growth into the esophagus;
- hiccups, shoulder pain - compression of the digestive nerve;
- spontaneous pneumothorax - ingrowth into the pleura.
Symptoms due to the general effect of the tumor on the body: general weakness, decreased ability to work, weight loss, increased body temperature.
Symptoms of extrapulmonary manifestations of cancer:
- arthropathy;
- muff-like thickenings of bones;
- pain in the bones, limited mobility in the joints;
- symptom of “drumsticks”, “watch glasses”. Cancer should be suspected when examining patients:
- with repeated transient pneumonia and “colds”;
- in the absence of an objective effect from anti-inflammatory treatment of pneumonia for 2-3 weeks;
- with polyarthritis that cannot be treated or with rapidly developing (over 2-3 weeks) symptoms of “drumsticks” and “watch glasses” in the absence of complaints from the respiratory system;
- with a sudden, for no apparent reason, “loss of voice” (Horner syndrome);
- all men over 50 years of age with pulmonary complaints;
- men with gynecomastia.
Laboratory and instrumental studies. General blood and urine tests, as well as a biochemical blood test, cannot provide any significant assistance in diagnosing lung cancer.
OAK: indicators characteristic of cancer - increases in ESR and lymphopenia - are variable and can be within normal limits even in advanced stages. Anemia, if it is not associated with hemoptysis, could be a manifestation of metastatic damage to the bone marrow, liver, or a consequence of cancer intoxication.
LHC: a decrease in the level of total protein, an increase in the level of bilirubin may be a reflection of a metastatic process.
Lung function tests and electrocardiography make it possible to confirm or exclude lung cancer.
Mandatory diagnostic methods for suspected lung cancer:
1. X-ray examination of the chest organs. A. Standard radiography or large-frame fluorography in frontal and lateral projections. Central cancer is characterized by the development of darkening of the entire lobe or segment with a decrease in the volume of the lung lobe.
and peripheral - a dense rounded shadow with a diameter of 1-5 cm, often in the upper lobes; B* Tomography; B. Contrast study of the esophagus to assess the mediastinal lymphatics.
2. Cytolomic examination of sputum (6-6 tests)
. Bronchoscopy with collection of material for morphological examination.
Among the special techniques used in specialized hospitals and oncology clinics are: radionuclide methods; additional x-ray examinations (computed tomography, bronchography, angiography of the bronchial arteries); surgical approaches (puncture or biopsy of subclavian lymph nodes, diagnostic thoracoscopy or thoracotomy); detection of tumor markers.
Speech restoration
This is the second important task of rehabilitation.
There are several rehabilitation programs. The choice is influenced by the period and stage of rehabilitation, the nature and degree of speech dysfunction. The main difference between the early stage and the late stage is the degree of patient participation: from passive to active.
What does the doctor do:
- Stimulates listening comprehension.
- Works with the expressive side of speech through the use of proverbs, songs, elementary speech patterns, and so on.
- Helps the patient complicate his speech with verbal vocabulary, which prevents agrammatism (telegraphic style).
- Engages the patient in reading and writing.
It is worth noting that restoration of speech function to its previous state is impossible. During treatment, the patient's speech changes its structure.
Lung cancer treatment
- Radical treatment is surgical (tumor removal in stages 1, 2, 3) in combination with radiation therapy.
- Palliative treatment is aimed at reducing the size of the tumor and prolonging the patient’s life:
- chemotherapy, cyclophosphamide, vincristine, taxol, etc.;
- symptomatic therapy: painkillers (from antispasmodics to narcotic analgesics), antihistamines (diphenhydramine, tavegil, suprastin) to potentiate the action of analgesics.
3. Patient care
in compliance with the rules of deontology. Hospitalization in a hospice in a terminal stage of illness.
Source: www.03-ektb.ru