© Author: A. Olesya Valerievna, candidate of medical sciences, practicing physician, teacher at a medical university, especially for SosudInfo.ru (about the authors)
The heart is one of the main “workers” of our body. Without stopping for a minute throughout life, it pumps a gigantic amount of blood, providing nutrition to all organs and tissues of the body. The most important characteristics of the efficiency of blood flow are the minute and stroke volume of the heart, the values of which are determined by many factors both from the heart itself and from the systems that regulate its functioning.
Minute blood volume (MBV) is a value characterizing the amount of blood that the myocardium sends into the circulatory system within a minute. It is measured in liters per minute and equals approximately 4-6 liters at rest with the body in a horizontal position. This means that the heart can pump all the blood contained in the vessels of the body in a minute.
Stroke volume of the heart
Stroke volume (SV) is the volume of blood that the heart pushes into the vessels during one contraction. At rest in the average person it is about 50-70 ml. This indicator is directly related to the condition of the heart muscle and its ability to contract with sufficient force. An increase in stroke volume occurs as the pulse increases (up to 90 ml or more). In athletes, this figure is much higher than in untrained individuals, even if the heart rate is approximately the same.
The volume of blood that the myocardium can throw into the great vessels is not constant. It is determined by the requests of authorities in specific conditions. So, during intense physical activity, anxiety, or in a state of sleep, organs consume different amounts of blood. The influences on myocardial contractility from the nervous and endocrine systems also differ.
As the heart rate increases, the force with which the myocardium pushes out blood increases and the volume of fluid entering the vessels increases due to the significant functional reserve of the organ. The reserve capacity of the heart is quite high: in untrained people, during exercise, cardiac output per minute reaches 400%, that is, the minute volume of blood ejected by the heart increases up to 4 times, in athletes this figure is even higher, their minute volume increases 5-7 times and reaches 40 liters per minute.
Stroke blood volume
Systolic or stroke volume characterizes the amount of total blood that one contraction of the cardiac ventricle throws into the arterial system. It is calculated using this simple formula: V = V * v. Where V is the systolic blood volume and v is the average beats per minute. Therefore, 70 * 70 = 4900 ≈ 5 liters per minute in normal health at rest is pumped by the heart.
But in reality, the indicator is individual for each person. Moreover, in women it is approximately 15% less. During physical activity, this number increases, and with heart problems or immobility, it decreases.
Steps
Heart rate detection
Take a stopwatch or watch.
Heart rate is the number of heartbeats per unit of time. It is usually measured in one minute. This is very easy to do, but you will need a device that will accurately count the seconds.
- You can try to count the beats and seconds mentally, but this will not be accurate because you will be focusing on your pulse rather than your internal sense of time.
- It's better to set a timer so you can concentrate only on counting the hits. There is a timer on your smartphone.
Find your pulse.
Although there are many places on the body where you can feel your pulse, the easiest place to find it is on the inside of your wrist. Another place is on the side of the throat, where the jugular vein is located. When you feel the pulse and clearly feel its beats, place the index and middle fingers of your other hand in place of the beat.
- Usually the pulse is best felt from the inside of the wrist, on a line mentally drawn from the index finger through the wrist and about 5 cm above the first fold on it.
- You may need to move your fingers back and forth a little to find where the pulse can be heard most clearly.
- You can press lightly on your wrist with your fingers to feel the pulse. However, if you have to push too hard, you have chosen the wrong place. Try moving your fingers to a different point.
Factors affecting stroke volume
What determines the amount of blood that the heart can pump into the bloodstream in one beat? There are several factors:
- Weight, physical development of the body.
- Having bad habits, in particular smoking.
- Pregnancy.
- Condition of the veins. Indicator of venous return to the right ventricle.
- Myocardial contractility.
- Preload.
In addition, the indicator depends on the size of the left ventricle of the heart. Those young people who have a small chamber of muscles from birth experience difficulties in training and often do not keep up with others.
The emission rate per minute is 4.5-5 liters. If CO decreases, then there is a high probability of atherosclerosis, arrhythmia or internal bleeding.
Relative_heart_volume
As already mentioned, the most important mechanisms ensuring an increase in cardiac performance (cardiac output) are an increase in the size of the heart (dilatation), an increase in myocardial contractility, and an increase in the efficiency of the heart. All these mechanisms are interconnected.
“Big (athletic) heart.” In representatives of endurance sports, the total volume of the heart, determined by radiographs, is on average significantly larger than in representatives of other sports and non-athletes).
Total and relative heart volumes, calculated from radiographs, in athletes of different specializations and in non-athletes (average data) (V.L. Karpman, S.V. Khrushchev and Yu.A. Borisova, 1978)
| Study population | Total heart volume, cm3 | Relative heart volume, cm3/kg |
| Male non-athletes | 11,2 | |
| Skiers | 15,5 | |
| Cyclists (road riders) | 14,2 | |
| Long distance runners | 15,5 | |
| Middle distance runners | 14,9 | |
| Swimmers | 13,9 | |
| Wrestlers | 12,2 | |
| Speed skaters | 12,5 | |
| Sprinters | 12,5 | |
| Gymnasts | 12,2 | |
| Weightlifters | 10,8 |
The total heart volume in endurance athletes exceeds 1000 cm3 (maximum up to 1700 cm3), while in other athletes it is not much more than in untrained people - about 800 cm3. Even greater differences are revealed in the relative volumes of the heart, that is, in the ratio of the total volume of the heart to body weight. In athletes who train endurance, the relative volume of the heart is on average 15 cm3/kg (maximum - up to 20 cm3/kg), and in untrained athletes it is about 11 cm3/kg. In athletes training endurance, a positive correlation is revealed between the total and relative volumes of the heart, on the one hand, and MOC, on the other. On average, the higher the sports qualification (sports result), the greater the heart volume of athletes of the same specialization.
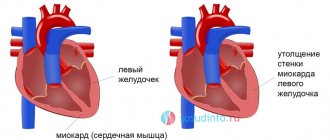
The overall size of the heart depends on the volume of its cavities and the thickness of their walls and therefore can change both due to dilation (increase in the size of the cavities) and due to myocardial hypertrophy (thickening of the walls of the cavities).
The hearts of endurance athletes are characterized by large ventricular divisions and normal or slightly increased ventricular wall thickness. Dilated ventricles are able to accommodate a large amount of blood during diastole, which creates the preconditions for increased systolic volume.
On the contrary, in representatives of speed-strength sports, the heart usually has normal or only slightly increased sizes of the ventricular cavities, but noticeable hypertrophy of the walls. The total cardiac volume of these athletes may exceed that of non-athletes, but the ability to increase systolic volume is almost the same in both.
Thus, cardiac hypertrophy is specific - its type is determined by the characteristics of training activity. Endurance exercise is characterized by repeated, but relatively small contractions of a large number of skeletal muscles and requires the maintenance of a large volume of cardiac output. In response to the action of such training stimuli, which can be called a “volumetric stressor,” the division of the heart cavities occurs with a large amount of blood, filling them and causing an increase in end-diastolic pressure. Therefore, this type of hypertrophy is called tonogenic dilatation (tonos - pressure). When performing speed-strength exercises, a strong short-term increase in blood pressure is necessary (“tension stressor”). In response to this stimulus, cardiac hypertrophy develops with thickening of the walls of the ventricles.
Myocardial hypertrophy is based on increased protein synthesis in myocardial fibers. Moreover, when training endurance in the heart, the synthesis of not only contractile proteins (actin, myosin, etc.) increases, but also proteins associated with its oxidative metabolism, in particular mitochondrial proteins and enzymes. At the same time, the number of capillaries increases, which improves the conditions of blood supply and aerobic metabolism of the heart muscle.
Efficiency of a dilated heart. Dilation of the heart gives it a number of energetic benefits. The dilated heart of an athlete allows to a greater extent: increase cardiac output by increasing systolic volume at a relatively low heart rate. This reduces the energy consumption of the heart and increases its mechanical efficiency compared to an untrained heart, which provides the same cardiac output due to a higher heart rate. In addition, the elongated myocardial fibers of a dilated heart develop greater tension with less shortening than fibers of a normal-sized heart (Frank-Starling mechanism). As a result, athletes with large cardiac volumes are able to maintain high systolic volume even at high heart rates.
Cardiac metabolism, as is known, proceeds almost exclusively along the aerobic pathway. Therefore, the work of the heart depends entirely on a constant and sufficient supply of oxygen and energy substances (glucose, fatty acids and lactate). The most important metabolic features of the trained heart in endurance athletes are as follows.
1. Due to increased capillarization and increased content of mitochondria and mitochondrial oxidative enzymes, the maximum rate of O2 delivery and utilization by a trained heart is greater than by an untrained heart.
2. With the same submaximal aerobic work, the blood supply and O2 consumption of a trained heart is less than that of an untrained heart. A higher partial tension of O2 in venous blood flowing from a trained heart indicates favorable conditions for the supply of oxygen to all myocardial cells.
3. A trained heart has an increased ability to extract lactate from the blood and utilize lactate. For the same arterial lactate concentration, the heart of an endurance athlete extracts more lactate than an untrained heart. If during maximum aerobic work the proportion of lactate among all oxidized energy substances in an untrained person can reach approximately 60%, then in a very endurance athlete it is more than 80%. In other words, the vast majority of the oxidative metabolism of a trained heart is covered by the use of lactate.
Cardiac output distribution, muscle blood flow and ABP-O2
High levels of aerobic capacity in trained athletes depend not only on high cardiac output, but also on the ability to use it more efficiently. This ability can be assessed by the value of systemic ABP-O2, i.e., the difference between the O2 content in arterial blood and in mixed venous blood flowing through the right heart. The greater the systemic AVR-O2, the more efficiently the body uses cardiac output, the more economically its oxygen transport system works. The O2 content in the arterial blood of trained athletes, either at rest or during aerobic exercise of any power, does not differ from its content in non-athletes. Therefore, an increase in systemic ABP-O2 as a result of endurance training can occur solely due to a decrease in the O2 content in mixed venous blood, i.e., due to a more complete use of O2 transported by the blood.
Factors for changing the IOC indicator
Minute blood volume (MBV) depends on the training and age of the person. IOC should be determined in order to find out how well the heart copes with its function.
The indicator primarily depends on three main characteristics:
- Heart rate;
- systolic volume;
- the magnitude of venous return.
To improve your performance, you need to pay attention to your lifestyle and think about prevention. With age, CO decreases greatly, and with any load, heart rate increases.
An athlete’s IOC can rise from 5 liters per minute to almost 20 liters. Such volumes can only be pumped by heart muscle prepared by long-term exercise.
Effect of afterload
As blood pressure rises or afterload increases, the volume of blood ejected may also increase. This property was documented and experimentally confirmed many years ago, which made it possible to make appropriate amendments to calculations and formulas.
If blood is ejected from the left ventricle under conditions of increased resistance, then for some time the volume of residual blood in the left ventricle will increase, the extensibility of myofibrils increases, this increases the stroke volume, and as a result, the minute volume of blood increases in accordance with the Frank-Starling rule. After several such cycles, the blood volume returns to its original value. The autonomic nervous system is an external regulator of cardiac output.
Ventricular filling pressure changes and contractility can alter stroke volume. Central venous pressure and the autonomic nervous system are factors that control cardiac output.
So, we have examined the concepts and definitions mentioned in the preamble of this article. We hope that the information presented above will be useful to all people interested in the topic discussed.
The heart muscle contracts up to 4 billion times throughout a person’s life, providing up to 200 million liters of blood into tissues and organs. The so-called cardiac output under physiological conditions ranges from 3.2 to 30 l/minute. Blood flow in organs changes, doubling, depending on the strength of their functioning, which is determined and characterized by several hemodynamic indicators.
Standard CO
We have already mentioned that for an ordinary person in a relaxed state, the normal systolic ejection volume is about 65-70 ml. It changes significantly when a person is actively involved in sports and does not miss training. Maximum CO is observed in track and field athletes during significant and prolonged physical activity.
The indicator often reaches 200 ml per systole. The athlete must control the systolic and minute blood volumes. To do this, you need to measure your heart rate before and after training.
How to accurately determine systolic and minute volumes?
The MOC can be more accurately determined using the following methods:
- Fick method.
- Ultrasonic flowmetry.
- Introduction of color indicators into the blood.
- Integral rheography. Rheography is a method in which the electrical resistance of the body to ultra-high frequency vibrations is recorded. These frequencies do not harm humans, therefore they are widely used in medical practice.
Systolic volume can be calculated by dividing minute volume by personal heart rate.
How to increase cardiac output?
To increase CO, athletes are advised to conduct long-term physical training of moderate intensity, during which the heart rate will not exceed 140-150 beats per minute.
Such loads will stretch the left ventricle, but will not increase the mass of the heart. It is prohibited to constantly build up your heart muscle through strength training alone. This is harmful to the organ and leads to a heart attack.
Ultrasound - norms and interpretation
Ultrasound examination of the heart
An ultrasound examination provides several indicators by which the doctor judges the condition of the heart muscle, in particular the functioning of the left ventricle.
- Cardiac output, normal 55-60%;
- The size of the atrium of the right chamber, the norm is 2.7-4.5 cm;
- Aortic diameter, normal 2.1-4.1 cm;
- The size of the atrium of the left chamber, the norm is 1.9-4 cm;
- Stroke volume, norm 60-100 cm.
It is important to evaluate not each indicator separately, but the overall clinical picture. If there is a deviation from the norm up or down in only one indicator, additional research will be required to determine the cause.
Heart failure in old age
In old age, if a person has moved little throughout his life, the walls of his heart become thinner, and the systolic volume does not exceed 20 ml. This is very little. The heart is not used to completely emptying the chambers, it weakens.
As a result, older people develop heart failure. When the valves are damaged, the heart cannot work at full strength, and then cardio training is dangerous.
It is necessary to lead a healthy lifestyle and walk outdoors more often. Hypokinesia (immobility) contributes to aging of the body, loss of strength and heart failure.
But the situation will be different if a person tries not to be lazy and goes to the gym. Training triggers a certain mechanism - an increase in negative pressure in the chest. This results in increased venous return to the heart.
Impact of training
For normal functioning of the heart muscle and valves, training is required. In physically developed people, the heart copes with the load thanks to good systolic volume without increasing the number of heartbeats per minute.
You need to exercise to the best of your ability. You should not allow your heart rate to exceed 190-200 beats per minute during cardio training.
Even unprofessional and irregular training has a positive effect on maintaining blood CO and helps the heart adapt to stress.
It must be said that systolic blood volume decreases with age. To maintain your health and physical strength, you need to run for 30 minutes every 2-3 days.