To dissolve a blood clot, enzyme preparations that can destroy fibrin strands are used. They are used in the first hours after a stroke, myocardial infarction, or pulmonary thromboembolism. Administration occurs in the usual intravenous manner or by local application of the medication to the blood clot. The most common and severe consequence of thrombolytic therapy is bleeding.
What it is?
Thrombolysis for myocardial infarction is a medical procedure for introducing into the human vascular bed one or another enzyme preparation that helps dissolve a blood clot that impedes normal blood circulation. Currently, a fairly large number of drugs used for thrombolysis therapy have been developed. Every year the number of these procedures in everyday medical practice is only increasing. This can significantly increase the survival rate and quality of life of patients with myocardial infarction. If thrombolysis was not performed, then after treatment, people often have to go on disability.
Methods of performing thrombolysis
Thrombolysis is carried out by two main methods:
local thrombolysis
- Systemic;
- Local.
The first method is advantageous in that the medicine can be injected into a vein without having any idea where the blood clot is hidden. With the bloodstream, the drug is carried throughout the entire blood circulation, where on its way it encounters an obstacle in the form of a blood clot and dissolves it. But systemic thrombolysis has a significant drawback: an increased dose of medication is required, and this is an additional burden on the entire circulatory system.
When performing local thrombolysis, the drug is injected directly into the location of the thrombus. The drug is supplied through a catheter, which is why the method is called catheter thrombolysis. However, this method is more difficult to implement than the first and is associated with a certain danger. During the procedure, the doctor monitors the movement of the catheter using x-rays. The advantage of this method is its low invasiveness. It is used even if the patient has a large number of chronic diseases.
Indications for use in myocardial infarction
Over time, the set of clinical conditions for which thrombolysis therapy is recommended is adjusted. Currently, the indications for thrombolysis for myocardial infarction are as follows:
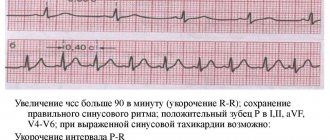
- the presence of ST segment elevation on electrocardiography, as well as other signs of acute myocardial infarction;
- no more than 12 hours from the time of onset of ischemic pain;
- the first complete blockade of the right bundle branch against the background of ischemic pain in the retrosternal region.
If all these conditions are met, then the medical professional begins to perform thrombolysis for myocardial infarction. An assessment of the possibility of carrying out this procedure should be carried out at the first contact of a patient with characteristic complaints with a medical professional.
Thrombolytic therapy for myocardial infarction
The article summarizes global experience in the use of thrombolytic drugs in acute myocardial infarction and provides data on the comparative effectiveness of various drugs for thrombolytic therapy. The main emphasis is on early initiation of treatment. Recommendations are given for correcting complications of thrombolytic therapy.
The paper summarizes worldwide experience in using thrombolytics in the treatment of acute myocardial infarction, provides evidence for comparative efficacy of different drugs for thrombolytic therapy. Great emphasis is laid on early treatment. Recommendations are given for correction of complications due to thrombolytic
therapy.
I.N. Bokarev, S.A. Dovgolis. Moscow Medical Academy named after. THEM. Sechenov IN Bokarev, SA Dovgolis IM Sechenov Moscow Medical Academy
AND
Myocardial infarction (MI) is the most common and dangerous pathological condition requiring emergency medical intervention.
Back in the early 60s, it led to the rapid death of 30-50% of those affected. The creation of intensive care units equipped with equipment for monitoring rhythm disturbances, combined with the introduction of electrical pulse therapy and new antiarrhythmic drugs, reduced mortality from MI by almost half. Thrombolytic drugs, which are currently the main ones in the treatment of MI, have made it possible in leading clinics in the world to reduce the mortality rate from this disease to 7% and even to 5%. Thrombolytic drugs were first used in clinical practice thanks to the efforts of V. Tillet and S. Sherry back in 1949, and in 1958 the same S. Sherry, together with A. Fletcher and N. Alkersig, already reported on the successful use of streptokinase (SK) for the treatment of patients with MI. However, the need for thrombolytic drugs for this pathology was recognized by everyone only after 1989. The undoubted merits of domestic scientists in the field of practical application of thrombolytic therapy are well known in the world. In 1961, domestic fibrinolysin, created by G.V. Andreenko under the leadership of B.A. Kudryashov, was first used in the clinic of A.L. Myasnikova E.I. Chazov. E.I. Chazov held the world priority for intracoronary administration of thrombolytic to a patient with MI in 1976. What is the situation with thrombolytic therapy for MI today, and what should every practitioner know about this? Thrombosis underlies MI in almost 95% of cases.
It usually develops after rupture of an atherosclerotic plaque.
Plaques with a large lipid core and macrophage infiltration of the fibrous surface are particularly susceptible to rupture. Myocardial cell death occurs in the direction from the subendocardium to the epicardium.
The main factors determining the final size of the infarction are the time to myocardial reperfusion and the development of collateral blood flow.
This determines the treatment tactics, the goal of which is to achieve early and sustained reperfusion of the occluded vessel, which will result in preservation of the myocardium, reduction in the spread of myocardial infarction and reduction in electrical instability of the myocardium. Restoring the patency of a damaged vessel helps to improve residual left ventricular (LV) function, reduce mortality, complications of MI, and improve survival. Reperfusion can limit the spread of MI in several ways. It reduces the amount to which the MI zone expands and the amount to which the perinfarction zone lengthens. Even in the absence of reduction in MI size, preservation of the epicardial layer may cause the affected area to be less distended. The healing pathway of the infarcted myocardium may be as important as the initial reduction in MI size. Late reperfusion of ischemic myocardial infarction also causes a decrease in muscle bundle necrosis and preservation of myocardial contractile function. Finally, reperfusion may reduce the risk of electrical instability. Early death in MI occurs suddenly as a result of ventricular fibrillation. Patients who have had reperfusion, according to electrophysiological studies, suffer less from ventricular arrhythmias, and they are less likely to have late repolarization disturbances on the ECG. The effect of reperfusion on reducing MI size is known to improve survival, but several factors appear to influence the deviation from the linear relationship between early reperfusion and mortality. For reperfusion to be most beneficial, it should not be very early, but long-term. Reocclusion is associated with a doubling of the risk of death. Differences between individual thrombolytic drugs in the rate of reocclusion are difficult to establish and require large studies. Several routes of administration of trobolytic drugs have been studied, from intracoronary thrombolysis to intravenous administration, both in hospitals and at home. Large clinical trials have clearly shown that intravenous thrombolysis is associated with a lower mortality rate in patients with acute chest pain and ST elevation within 12 hours of symptom onset.
Evidence of effectiveness.
| Currently, the following types of thrombolytic agents are used in the world: streptokinase (SK), urokinase, acylated plasminogen-SK complex (APSAC) and tissue plasminogen activator (tPA). The latter has some advantages, but the high cost of the drug limits its use. |
Domestic fibrinolysin turned out to be less effective and is currently not produced. Comparative studies of thrombolytic therapy with placebo have clearly shown a reduction in mortality of 25-30%, regardless of the thrombolytic drug used. Currently, 10 large prospective randomized trials have been conducted to evaluate the effect of early thrombolysis on mortality. The GISSI-1 trial (the first Italian cooperative trial of thrombolytic agents in MI), a large study on early intravenous thrombolysis, was a milestone that marked the beginning of the era of routine use of thrombolytic drugs in patients with early acute MI (AMI). In this study, 11,712 patients admitted within the first 12 hours of AMI and who had no contraindications to thrombolytic therapy were randomized to receive treatment with an intravenous infusion of 1,500,000 U of SA over 1 hour or usual treatment without SA. Mortality at 21 days in the group receiving SA was 10.7% compared with 13% in the control group (decreased mortality by 18%, p = 0.0002). No effect was observed in patients treated with SC later than 6 hours from the onset of pain. Those treated within 6 hours had a mortality rate of 10.2% compared with 12.8% in the control group (20% reduction in mortality). The earlier treatment was started, the higher its effectiveness. Thus, in patients who began treatment within 3–6 hours, SC led to a reduction in mortality by 17% (from 14.1 to 11.7%). If it was started between 0 and 3 hours, the reduction in mortality was 23% (from 12 to 9.2%). In those treated within 1 hour from the onset of symptoms, the reduction in mortality reached 47% (from 15.4 to 8.2%). ISIS-2 (the second international MI survival study) was also very important. The investigators reported baseline and final data on 17,187 patients with suspected AMI who were enrolled within 24 hours of pain onset. Patients were randomized in a double-blind manner. The effect of intravenous administration of SA (1,500,000 units over 60 minutes) or oral aspirin (160 mg per day for 1 month), or both, was studied. Patients were excluded from the study if more than 24 hours passed from the onset of symptoms. There were no age restrictions. We studied the effect of SC on the level of cardiovascular mortality for 5 weeks and later, the effect on cardiovascular mortality for 5 weeks. In addition, we analyzed the effect of SC on cardiovascular mortality in those treated earlier than 4 hours from the onset of pain, in those treated in the period 4–12 hours and in the period 12–24 hours. When analyzing mortality for 5 weeks from the moment of inclusion, it was found that from Of the 8592 patients treated with SK, 786 (9.1%) died of cardiovascular causes compared with 1016 of the 8592 patients treated with placebo (23% reduction in mortality, P < 0.00001). This difference is comparable to the 18% reduction in mortality in the GISSI-1 study. Over the period from 5 weeks to 1 year, the mortality rates in the SC and placebo groups were 5.7 and 6.2%, respectively. In ISIS-2, only 56% of patients had ST elevation at baseline, 8% had ST depression, 6% had bundle branch block, 27% had Q-wave or T-wave inversion, or both, 2% The ECG was normal. The GISSI-1 and ISIS-2 studies, as well as studies conducted in the Netherlands, Germany, New Zealand, and Washington State, provided convincing evidence that SA, administered early in the course of myocardial infarction to patients without contraindications, reduces mortality by 20-30%. Similar data were obtained for tPA and APSAC. In the ASSET study (English-Scandinavian Early Thrombolysis Study), 5011 patients with suspected AMI received 100 mg alteplase (rTPA; 10 mg bolus, 50 mg in the 1st hour, 20 mg in the 2nd hour) in the first 5 hours after the onset of the disease after randomization. 1st and 3rd hour) or placebo. ASSET did not adhere to ECG criteria for the diagnosis of MI, but excluded patients over 75 years of age. About 18% of patients had a normal ECG upon inclusion in the study. At 1 month, the overall mortality rate in the treatment group was 7.2% compared with 9.8% in the placebo group (26% reduction in mortality, P = 0.0011). The European Cooperative Group reported a randomized, double-blind study of rTPA (100 mg) in 721 patients with chest pain and ST-segment elevation within 5 hours of pain onset. Both groups received aspirin and heparin. Researchers studied the effect of treatment on LV function. Death within 14 days and death within 3 months were adopted as secondary endpoints. 14-day mortality was 2.8% (10 of 355) in the rTPA group and 5.7% (21 of 366) in the placebo group. There was a 51% reduction in mortality (p = 0.06). Ejection fraction (EF) was 2.2 times higher in the rTPA group compared to the placebo group (50.7 and 48.5, respectively). MI size, assessed by total hydroxybutyrate dehydrogenase release, was 20% smaller in the hTPA group (p = 0.0018). The British AIMS research group conducted a multicenter, double-blind, placebo-controlled study of the effect of APSAC (30 units intravenously over 5 minutes) in patients under 70 years of age who were admitted within 6 hours of the onset of ST-segment elevation pain on the ECG. The data monitoring committee recommended early termination of the study after reanalysis of the interim data when 50% of the expected number of patients had been recruited. In a preliminary report of 1004 patients, 30-day mortality was 12.2% (61 of 502) in the placebo group and 6.4% (32 of 502) in the APSAC group (p = 0.0016). The overall reduction in mortality among patients included in the study in the interval 4–6 hours from the onset of the disease was 47%; the decrease was significantly greater in those included in the study in the first 4 hours (52 and 41%, respectively). The overall benefits of treatment are maintained and even increased between 30 days and 1 year. Mortality at 1 year was 19.4 and 10.8%, respectively, in the placebo and APSAC groups (44% reduction in mortality; P = 0.0006). However, there is evidence that KS and APSAC therapy are equally effective. Two studies, the European Cooperative Study and TIMI (Thrombolysis in Myocardial Infarction), compared the effects of rTPA and SC on arterial patency or reperfusion rates. In the European Cooperative Study, 129 patients received either rTPA or SC an average of 3 hours after the onset of MI. The patency of the infused artery was studied 90 minutes after the start of the infusion; it was 70 and 55%, respectively (p = 0.058). The TIMI study also used rTPA and pretreatment arteriography. The authors observed 70 and 43% arterial patency rates 90 minutes after the start of rTPA and SA infusion, respectively, in 290 patients treated on average 4.75 hours after the onset of pain. In summary, arterial patency rates in the two studies were identical for gTAP (70%) and minimally different for MC (55% in the European Cooperative Study and 43% in TIMI). In the TIMI study of 232 patients with an occluded artery, reperfusion within 90 minutes was observed in 62 and 31% of patients treated with rTPA and SA, respectively. In both studies, changes in the coagulation system were insignificant when using rTPA, although hemorrhagic complications were observed during treatment with both SC and rTPA (mainly the formation of hematomas at the site of arterial puncture). The conclusion is clear: under the influence of rTPA and SC, thrombolysis occurs, followed by reperfusion, limiting the size of myocardial infarction and improving LV remodeling, which is obviously a mechanism for reducing mortality. There is a linear relationship between mortality and the time from symptom onset to initiation of thrombolytic therapy.
The FTT (Fibrinolytic Therapy Trialists) study showed a dependence only up to 12 hours from the onset of symptoms. Within 1 hour after the onset of symptoms, the effect of thrombolytic drugs is less significant; its maximum was detected when the drug was administered 2–3 hours after the onset of the disease. The benefit of treatment then clearly decreases with increasing time from symptom onset. The effect of late thrombolysis in AMI, i.e. treatment started after 6 hours from the onset of symptoms, remains not entirely clear. In the ISIS-2 study, among patients treated within the first 4 hours, the mortality rate in the SA and placebo groups was 8.2 and 12.1%, respectively (a 32% reduction). Among patients treated in the period 4 - 12 hours, mortality from cardiovascular causes was 10.3 and 11.8%, respectively (a decrease of 13%) and among patients treated in the period 12 - 24 hours - 10.7 and 10.8% (0.9% decrease). Among patients treated within 1 hour, 5-week mortality in the SC group was reduced by 42% (similar to the 47% reduction in 3-week mortality in the GISSI-1 study). The LATE (Delayed Thrombolysis Impact on Survival in MI) study, designed to address the benefit of late thrombolysis with tPA, showed the following. 5711 patients with symptoms and ECG parameters consistent with AMI were randomized to receive alteplase (100 mg IV over 3 hours) or placebo between 6 and 24 hours from the onset of symptoms. Both groups of patients received aspirin. They were followed up for 6 months, and 73% for 1 year. Survival analysis revealed a reduction in mortality in the alteplase group (397/2836 deaths) compared with placebo (444/2875). The 35-day mortality rate was 8.86 and 10.31%, respectively, a relative decrease of 14.1%. Additional survival analysis for treatment up to 12 hours from symptom onset showed a significant reduction in mortality with alteplase: mortality at 35 days was 8.9% versus 11.97% for placebo, a relative reduction of 25.6% (p = 0.0299) . For those treated between 12 and 24 hours, the mortality rate was 8.7 and 9.2%, respectively, suggesting that there may be some benefit from treatment beyond 12 hours. This study showed that the start time of alteplase thrombolysis can be extended to 12 hours from the appearance of AMI symptoms.
| The benefit of fibrinolytic therapy was observed in all except patients with ST depression. The absolute benefit was greatest in subgroups with the greatest risk, as determined by hemodynamic markers of large infarcts or general factors such as older age. Studies have shown that the degree of ST elevation is a marker of the potential benefit of thrombolytic drugs. Patients with greater ST elevation should expect the greatest benefit from this treatment. |
The question of the dependence of the effectiveness of thrombolytic therapy on the localization of myocardial infarction
seemed important, since it is almost always possible to accurately determine the localization of MI: anterior, lateral, inferior or circular, depending on the location of ST elevation on the first ECG.
It is much more difficult to detect the presence of a true inferior Q-infarction in patients admitted with ST depression in the anterior wall. The GISSI-I study and others found that anterior MI has a higher mortality rate and therefore patients with anterior MI benefit most from thrombolytic therapy. The effectiveness of thrombolytic therapy in patients with lower myocardial infarction is less clear in the GISSI-1 study, but benefit from the use of SA and aspirin was shown in ISIS-2. Patients with anterior MI who received thrombolytic therapy showed a 30% reduction in mortality compared with 15% in patients with inferior MI. At the same time, many clinicians believe that thrombolytic therapy is indicated for patients with hypotension, cardiogenic shock, especially patients with inferior MI and right ventricular involvement. An analysis of the effectiveness of thrombolytic therapy depending on age
showed the following.
In patients under 55 years of age, the risk of life without thrombolytic therapy is not very high. The absolute benefit of treatment increases with patient age. Almost 50% of all deaths of patients hospitalized for AMI occur in the age group over 75 years. In studies of thrombolytic therapy, in addition to ISIS-2 and GISSI-1, patients over 70 years of age (AIMS) or 75 years of age (ASSET, Eur. Coop. Study) were excluded. The ISIS-2 study showed a reduction in mortality with the use of SC by 16% over 5 weeks (18.2 and 21.6%) in the group of patients over 70 years of age, by 26% (10.6 and 14.4%) in the group of patients 60-69 years old and by 28% (4.2 and 5.8%) in the group of patients under 60 years old. The GISSI-1 study reported a 13% reduction in mortality at 3 weeks in the group of patients over 75 years of age, by 8% in the group of 65-75 years, and by 26% in the group not older than 65 years. It also shows that the risk of bleeding does not depend on age. Currently, work is underway to objectify the effectiveness of old and create more effective new thrombolytic drugs.
To prove the benefits of a new drug over its predecessors in the same class, a study involving at least 20,000 patients is required. Two large studies, GISSI-2 (20,891 patients) and ISIS-3 (41,229 patients), were designed to determine the benefits of alteplase over SK (GISSI-2) or alteplase and anistreplase over SK (ISIS-3). Both studies found similar mortality rates when treated with different thrombolytic agents. The use of SA was accompanied by a significantly lower incidence of strokes compared to that with the use of anistreplase and alteplase.
Frequency (in%) of adverse events during thrombolytic therapy
| Complication | GISSI-1 (5860; UK) | ISIS-2 (8592; UK) | ASSET (2512; TAP) |
| Major bleeding | 0,3 | 0,5 | 1,4 |
| Minor bleeding | 3,7 | 3,5 | 6,3 |
| Allergic reaction | 2,3 | 4,4 | 0 |
| Anaphylaxis | 0,1 | 0 | 0 |
| Hypotension | 3,0 | 10,0 | HP |
| Stroke | 1,1 | 0,7 | 1,1 |
| Intracranial pressure | HP | 0,1 | 0,3 |
Note. HP - not registered.
The INJECT trial aimed to determine whether the new drug reteplase (recombinant plasminogen activator) has the same effect on mortality as CK. 6010 patients were randomized to receive reteplase (3004 patients) or SK (3006 patients). Both treatment groups achieved similar results over 6 months in terms of the incidence of bleeding episodes, extension or recurrence of myocardial infarction, and in-hospital strokes with subsequent disability. Those treated with reteplase had fewer cases of ischemia and slightly more allergic reactions. The number of diagnosed strokes was higher among those treated with reteplase, but strokes also occurred in a number of patients treated with SA. Mortality within 35 days in patients treated with reteplase was approximately 0.5% lower than in patients treated with KS. Two angiographic studies, RAPID 1 and RAPID 2, involving 324 patients, assessed vessel patency after AMI when treated with reteplase or alteplase. The RAPID 1 study examined different dosing regimens of reteplase compared with a 3-hour infusion of alteplase. The RAPID 2 study compared a double bolus regimen of reteplase with an accelerated infusion (90 min infusion) of alteplase. The results of these studies showed that reteplase opens more arteries faster than alteplase. Angiography at 60 and 90 minutes showed a higher level of patency and a 3-fold higher level of myocardial perfusion with reteplase compared with those with alteplase. In RAPID 1, after 90 minutes, the perfusion level was 63% for reteplase compared to 49% for alteplase (p < 0.05); in RAPID 2, the perfusion level was 60 and 45%, respectively (p < 0.05). Reteplase was more convenient and easier to use, and there were no unexpected complications. The angiographic profile for reteplase demonstrated in these two studies suggests that this new thrombolytic agent has advantages over alteplase; notably, its use may result in earlier and more complete coronary artery patency. Two recent studies from Europe, the GREAT (Anistreplase Early Treatment Trial) and EMIP (European MI Project), demonstrate the feasibility, safety and effectiveness of early thrombolytic therapy before hospital admission. In the GREAT trial, anistreplase (APSAC) was administered by a general practitioner at home. At EMIP, the same drug was administered by emergency personnel. In both studies, prehospital administration reduced the time between symptom onset and initiation of thrombolytic therapy and was associated with lower mortality rates. Recent data from a European Cooperative Group study showed that the benefit of thrombolytic therapy lasts for at least 5 years. Additional benefits can be obtained by using new methods of thrombolysis, which consist in accelerated administration of thrombolytic drugs, in particular SA and tPA.
In 1993, the GUSTO (Global Use of SK and TPA in Occluded Arteries) trial enrolled 41,021 patients; these patients were randomized to receive alteplase (accelerated administration) and intravenous heparin; a combination of alteplase, SA and heparin intravenously; SA and heparin intravenously; SC and heparin subcutaneously. For the first time, it was shown that a new method of thrombolytic therapy, consisting of accelerated administration of tPA, reduces mortality by another 15% compared with SC and slightly increases the risk of intracranial hemorrhage. The researchers obtained expected and unexpected results. The accelerated tPA administration regimen was accompanied by a rapid restoration of perfusion and blood flow of TIMI grade III compared with any SA administration regimen. Numerous measurements have shown better LV systolic function after accelerated tPA administration. In addition, with accelerated tPA administration, mortality rates were lower at 30 days and at 1 year, equivalent to 10 and 11 lives saved per 1000 patients treated. We also reported similar observations in the treatment of 190 patients admitted for acute MI with a Q wave in the first 6 hours from the onset of the disease. All patients received thrombolytic therapy with SK. 160 patients (Group 1) were administered SA according to the standard method (1,500,000 units intravenously over 1 hour), and 30 patients (Group 2) were administered according to a rapid regimen (750,000 units in 20 ml of saline over 5 – 7 min). Thrombolysis was found effective in 110 (68.8%) patients of group 1 and in 25 (83.3%) patients of group 2. Early rethrombosis (up to 180 minutes) occurred in 7 (4.4%) and 2 (6.7%) cases, respectively. Hospital mortality was 15 (9.4%) cases in the 1st group and 2 (6.7%) cases in the 2nd group. There were no significant differences between the groups in the incidence of recurrent AMI, acute aneurysm, angina, circulatory failure, arrhythmias and blockades. Currently used thrombolysis methods do not guarantee myocardial reperfusion. Early and complete reperfusion is achieved in less than 50% of patients 90 minutes after the start of treatment, and reocclusion occurs in approximately 20–25% of patients during the 1st year of observation. Moreover, only 3–4% of patients receive a thrombolytic drug within the 1st hour of symptom onset, when benefit may be greatest. Therefore, the need to improve approaches to the treatment of AMI is beyond doubt.
Scheme of thrombolytic therapy for MI
Indications
• Chest pain, typical of acute myocardial ischemia, lasting up to 12 hours. The pain is not relieved by nitrates and has no obvious cause of noncardiac origin. After 12 hours, thrombolysis should be performed in patients with the most unfavorable prognosis, in whom the greatest benefit can be expected (over 75 years of age, in cases of extensive damage, ongoing anginal pain, arterial hypotension). In these cases, you can expect to save 10 lives per 1000 treated. • ECG changes: – recently or presumably recently appeared Q waves lasting more than 0.03 s with an amplitude of more than 0.2 mV; these changes should be noted in 2 of 3 “lower” (II, III, aVF) or 2 of 6 precordial (V1 – V6) leads or in I and aVL; – recently or supposedly recently appeared ST elevation of 0.1 mV or more; ST elevation is measured at a distance of 0.02 s from the end of the S wave; – bundle branch block. If systolic blood pressure exceeds 180 mm Hg. Art., you first need to achieve its reduction, preferably with the help of intravenous atenolol or labetalol.
Contraindications
• Absolute: – bleeding at the time of examination; - stroke; – gastrointestinal bleeding during the last month; – recent (in the previous 3 weeks) major surgery, major trauma or head injury; – dissecting aortic aneurysm; – known hemorrhagic diathesis. • Relative (the possible risk must be carefully weighed against the benefit): – transient cerebral ischemia in the previous 6 months; – treatment with oral anticoagulants – antivitamins K; – pregnancy; – recent traumatic cardiopulmonary resuscitation (more than 10 minutes); – refractory arterial hypertension (BP > 180/100 mm Hg); – recent puncture of a non-compressible vessel; – recent retinal laser treatment.
Methodology
It is desirable that the interval from the patient’s admission to the hospital to the start of thrombolytic therapy does not exceed 30 minutes. Intravenous administration of SA is carried out as follows: 1,500,000 units are administered in 100 ml of 5% glucose or 0.9% sodium chloride over 30–60 minutes. The administration of heparin is not necessary; subcutaneous administration of 12,500 units 2 times is possible. Specific contraindications are previous (up to 5 days) use of SA or anistreplase. TPA (alteplase) is administered according to the following scheme: 15 mg of the drug intravenously as a bolus, then 0.75 mg/kg over 1 hour intravenously over 30 minutes, then 0.5 mg/kg over 1 hour; total dose 100 mg. Heparin is administered intravenously over 48 hours. APSAC (anistreplase) is administered at a dose of 30 units intravenously over 5 minutes. Specific contraindications include prior use of SA or Anistreplase 5 days prior and known allergy to SA/Anistreplase. Urokinase is administered at a dose of 2,000,000 units intravenously as a bolus or 1,500,000 units as a bolus + 1,500,000 units over 1 hour. Heparin is administered within 48 hours. If signs of reocclusion or repeated MI with ST elevation or bundle branch block appear, it should be repeated perform thrombolysis or angioplasty. During the period from 5 days to 2 years, SC or APSAC should not be reused. Antibodies to KS persist for at least 2 years. The use of alteplase and urokinase does not lead to the formation of antibodies. Evaluation of the effectiveness of thrombolytic therapy
There are several markers of success of thrombolytic therapy. A decrease in ST elevation in 12 standard ECG leads 1 to 4 hours after the start of thrombolysis is the simplest and most useful clinical sign for assessing the effectiveness of thrombolytic therapy. The predictive value of this indicator can be enhanced by combining it with serum myoglobin and troponin T levels, which can be rapidly determined. Additional signs of the effectiveness of thrombolytic therapy may be the cessation of anginal pain and a significant (40–100%) increase in the activity of enzymes, primarily creatine phosphokinase. The appearance of reperfusion arrhythmias - accelerated idioventricular rhythm, ventricular extrasystoles, ventricular tachycardia, ventricular fibrillation, atrioventricular (AV) blockade, etc. - can also be taken into account, but can also be considered as a complication. It should be noted that the contractility of the myocardium during reperfusion is not immediately restored (the phenomenon of “stunned myocardium”).
Complications
Thrombolytic therapy may be accompanied by adverse reactions. The likelihood of complications depends on taking into account absolute and relative contraindications, the choice of drug and the method of thrombolytic therapy. Reperfusion arrhythmias, a common complication of thrombolytic therapy and at the same time indirect evidence of its effectiveness, are observed in 20–60% of patients. The most common are accelerated idioventricular rhythm, ventricular extrasystoles, paroxysms of unstable ventricular tachycardia, transient AV block, and ventricular fibrillation. Treatment of arrhythmias is carried out according to the same principles as similar rhythm and conduction disorders not associated with reperfusion. Reocclusion of the coronary artery is observed in 15–20% of cases and is often asymptomatic. In some patients, reocclusion is manifested by the resumption of anginal pain and deterioration of hemodynamics. To prevent and treat this complication, nitroglycerin and heparin are administered intravenously. Hypotension is usually corrected by the rate of administration of the thrombolytic drug. If this is not enough, then infusion therapy and corticosteroid hormones are prescribed (prednisolone 30–60 mg, and if there is no effect, dopamine 2–5 mcg/kg per minute). Allergic reactions require immediate cessation of administration of the thrombolytic drug and, depending on the clinical manifestations, the prescription of antihistamines, corticosteroid hormones, bronchodilators, and in the event of anaphylactic shock, adrenaline. If there is a need for pacing or hemodynamic monitoring, it is advisable to do this before initiating thrombolytic therapy. Puncture of the subclavian or internal jugular vein is contraindicated. A serious complication of thrombolytic therapy is intracranial hemorrhage. Widespread adoption of new routes of thrombolytic drug administration has been hampered by the concern that improved reperfusion may lead to an increased incidence of intracranial hemorrhage. They are more often observed when using fibrin-specific agents compared to SC. This was demonstrated in the studies GUSTO 2 A, TIMI 9 and HIT 3. Hemorrhagic stroke usually develops in elderly patients with uncontrolled arterial hypertension and a burdened neurological history, therefore thrombolytic therapy is contraindicated in this category of patients. If a hemorrhagic stroke develops, its treatment is carried out in the same way as without thrombolytic therapy. At a dose of SA of 1,500,000 units per 1 hour, the risk of intracranial hemorrhage is 1–10 per 1000 treated patients. Gastrointestinal bleeding of varying severity can be expected in 5% of patients, genitourinary bleeding - with the same frequency. The incidence of intracranial hemorrhage after rTPA is dose dependent. At a dose of 150 mg it is 15–20 per 1000, and at a dose of 100 mg it is 5–10 per 1000. Intracranial hemorrhages with the use of APSAC are not clearly recorded. Even with effective thrombolysis, there remains an increased risk of ischemia because atherosclerotic plaque remains. In this regard, patients remain at risk of relapse and repeated MI in the future. In some patients, despite therapy with aspirin and heparin, after successful thrombolysis, chest pain and repeated coronary artery thrombosis with the development of MI reappear. Coronary thrombolysis has little effect on those hemodynamic factors in the coronary artery affected by atherosclerosis, which contribute to the activation of fibrinogen and the formation of a blood clot; it only restores coronary blood flow for some time. After successful thrombolysis, patients are advised to undergo emergency coronary artery bypass surgery or balloon angioplasty with stent placement in order to prevent recurrent coronary artery thrombosis. Fluctuations in the risk of AMI throughout the day are likely due to diurnal fluctuations in coagulation activity and the effect of getting out of bed after sleep. Whether the different balance between coagulation and fibrinolysis at the physiological level influences the effect of thrombolytic drugs remains unclear. Attempts are being made to develop safer and more effective thrombolytic agents. Public awareness of the symptoms of MI and the development of a faster and more effective emergency response system may also improve the outcome of thrombolytic therapy by shortening the time between the onset of symptoms and administration of the thrombolytic drug. A modern doctor should know that the earliest administration of a thrombolytic drug to a patient with MI is the best way to save a person and ensure the safety of hemodynamics.
Recommended reading:
1. Alpert J., Francis G. Treatment of myocardial infarction. Practical guide. Per. from English – M.: Praktika, 1994. – P. 196–201. 2. Bokarev I.N., Pavlov A.V., Yankin V.V., Kazharskaya E.E., Dovgolis S.A., Inokentyev I.K., Martynova I.G., Lando L.G., Fedorova S.Yu., Lepersky A.L., Blokhina I.V., Ulybysheva M.A. Rapid thrombolysis with streptokinase drugs in acute myocardial infarction. /Thrombosis, hemorrhages, DIC syndrome. Treatment issues. International Conference. Moscow. April 2–4, 1997 3. Cardiology in tables and diagrams. Ed. M. Frida and S. Grines. Per. from English - M.: Praktika, 1996. – P. 149–50. 4. International guidelines for myocardial infarction. Ed.
Absolute contraindications
This procedure is considered quite complex and is not always easily tolerated by patients. Doctors have established a whole list of conditions that may interfere with its implementation. Today, the following absolute contraindications to thrombolysis for myocardial infarction are identified:
- Presence of dissecting aortic aneurysm.
- History of hemorrhagic stroke less than 6 months ago.
- Disorders of the blood coagulation system.
- Arterial hypertension resistant to antihypertensive therapy (with the help of medications it is not possible to reduce the level of systolic blood pressure below 220 mm Hg, and diastolic blood pressure below 110 mm Hg).
- Surgery less than 3 weeks ago.
- Gastrointestinal bleeding less than 1 month ago.
- Traumatic brain injury less than 3 weeks ago.
For all these conditions, thrombolysis therapy is not performed. This is due to the fact that the risk of developing serious, life-threatening complications is greater than the positive effect of the procedure.
Thrombolysis results
Not only thrombolysis helps doctors save the life of the injured person and restore blood circulation in the vessels. Some other methods also give a similar effect. Studies have shown that timely thrombolysis:
- promotes a speedy recovery,
- reduces the length of hospital stay,
- increases the chances of maintaining working capacity after a heart attack.
Although during a heart attack the diseased cardiovascular system fails, it is possible to restore its functioning. If qualified doctors do this, the result is guaranteed.
Relative contraindications
There are situations in which thrombolysis therapy is undesirable, but is possible in cases where the expected benefit of the procedure outweighs the possible harm from it.
Today, the following relative contraindications to thrombolysis for myocardial infarction are identified:
- Transient ischemic attacks less than 6 months ago.
- Pregnancy.
- Postpartum period (less than 28 days after resolution of pregnancy).
- Constant use of direct anticoagulants.
- Prolonged cardiopulmonary resuscitation, accompanied by trauma to the patient.
- The presence of gastric ulcers in the acute stage.
- Liver failure.
- Infectious endocarditis.
- Puncture of large vessels that are inaccessible for compression.
- Any hemorrhages in the retina.
Despite the large number of relative contraindications, doctors most often perform thrombolysis for myocardial infarction, regardless of their presence, since without this procedure there is a high probability of developing the most severe consequences for patients.
Types of thrombolysis
There are two types of thrombolysis: early and late. Late thrombolysis is considered to be performed within 3-6 hours after blockage of blood vessels by a thrombus. It restores blood supply to the heart, supports the functioning of the left ventricle and prevents the development of death. The most effective is early thrombolysis, which is carried out in the first hours of a heart attack.
Indications for thrombolytic therapy include:
- The first 12 hours from the onset of pain.
- The presence of an attack of acute pain in the chest area, which lasts more than 30 minutes.
- Registration of ST segment elevation on the ECG.
- Detection of signs of complete blockade of the left bundle branch on the electrocardiogram.
Possible side effects
This procedure is often quite difficult for the patient. Adverse reactions develop in approximately 1% of patients undergoing thrombolysis for myocardial infarction. Some of the most common side effects include:
The complexity of the procedure, as well as the possible development of side effects, are some of the reasons why thrombolysis for myocardial infarction is most often performed in the intensive care unit (if the patient is an inpatient).
Complications after thrombolysis
Complications of thrombolytic therapy include:
- Bleeding of varying intensity and localization.
- Impaired myocardial contractile function and the development of heart failure.
- Allergic reaction and development of anaphylactic shock.
- Cerebral hemorrhagic stroke.
- Reperfusion (associated with return blood flow from the atria to the aorta) cardiac arrhythmias.
- Repeated blockage of heart vessels.
- Persistent decrease in blood pressure.
- Increased body temperature, chills and rash.
Cerebral hemorrhagic stroke more often develops in individuals with risk factors, which include:
- Use of alteplase in thrombolytic therapy.
- High blood pressure levels.
- Patient age greater than 65 years.
- The patient's weight is less than 70 kilograms.
Thrombolysis helps restore blood flow and provides nutrition to the heart muscle. In most cases, thrombolysis prevents death and saves the life of patients.
Criteria for the success of the procedure
If thrombolysis is carried out successfully, the following phenomena are observed:
- The patient's pain quickly decreases and then disappears.
- Return of electrocardiography parameters to normal.
- Development of atrial fibrillation (atrial fibrillation) during thrombolytic therapy.
- Return to normal levels of cardiac-specific biochemical markers of necrosis.
Also, during thrombolysis, the patient’s general condition and other indicators of his health (heart rate, respiration, blood pressure level, etc.) are assessed.
Progress of the procedure
Thrombolytic therapy for a heart attack is carried out either by emergency doctors or in the intensive care unit. After the patient is admitted to the hospital, all preparatory measures must be carried out within an hour. During this time, the patient must be examined for concomitant diseases and the presence of contraindications to the procedure.
Myocardial infarction is a dangerous pathology in which every minute can save a person’s life. When performing thrombolysis, the doctor should adhere to the following recommendations:
- Before administering thrombolytic drugs, urinary catheters are installed;
- During the first days after treatment, catheters should not be inserted into large arteries;
- During the day, any intramuscular injections are prohibited;
- When selecting a dosage, the patient’s weight should be taken into account.
Also read: How to prevent a heart attack?
Age is not a contraindication for the use of thrombolytics. The less time has passed since the onset of the attack, the greater the effect of the therapy. This is due to the fact that fresh blood clots have a softer consistency and are more easily absorbed. Over time, they become denser, which makes the treatment process much more difficult.
For thrombolytic therapy use:
- Puroplase is a recombinant prourokinase.
- Alteplase. This is a fibrin-specific antigen. It is administered after 4 hours.
- Tenecteplase. The drug is used for management in the prehospital period.
Also, during the treatment process, Actilyse is often used in the following dosage:
- During the first three hours, a string injection of 15 mg of Actilyse is administered. After this, 50 mg is administered by infusion. After an hour for 60 minutes - another 35 mg of the substance. Do not administer more than 100 mg of the drug.
- If treatment takes place within 6 to 12 hours, then first 10 mg is administered by string method, then 59 mg is administered by infusion. Then 10 mg are administered every half hour until the total dosage reaches 100 mg.
The doctor who performs the procedure must strictly follow the instructions.
Drugs for thrombolysis
Over the past decades, the main drug for thrombolysis therapy was the drug “Streptokinase”. It belongs to the group of direct tissue plasminogen activators. This drug is relatively cheap, but it is not effective enough, and it often causes serious side effects. Currently, indirect tissue plasminogen activators are becoming increasingly widespread, the main of which are:
Thrombolysis in myocardial infarction carried out with indirect tissue plasminogen activators often occurs without negative reactions and has good effectiveness. Their main disadvantage is the relatively high cost in comparison with the drug "Streptokinase".
What is thrombolysis
Thrombolysis is a process aimed at dissolving a blood clot formed in a blood vessel. In the body of a healthy person, it occurs constantly, preventing the formation of small blood clots. The dissolution process occurs with the help of special enzymes.
If large blood clots have formed, the body is unable to dissolve them on its own. At best, a small hole may appear in the clot, but this is not enough for normal blood circulation.
As new blood clots form, nutrition to vital organs deteriorates, and the risk of heart attack (death of heart muscle cells) increases. If nothing is done, necrosis begins in the tissues, and muscle contraction worsens, which can lead to sudden cardiac arrest.
Important! Thrombolysis is carried out by doctors in a hospital or emergency room. The essence of the method is to administer drugs that can dissolve a blood clot in the shortest possible time.
Timely thrombolysis can stop myocardial infarction, protecting most of the heart muscle. The procedure fully restores blood supply and nutrition to heart cells.
Mechanism of action of drugs
These drugs ensure the binding of the enzyme to plasminogen located on fibrin. Under the influence of drugs, plasminogen is converted into plasmin, penetrating fibrin. Subsequently, plasmin destroys fibrin, thereby ensuring the disintegration of the blood clot.
When performing thrombolysis, microthrombi may form. Also, the introduction of tissue plasminogen activators helps to increase platelet activity. All this requires concomitant antiplatelet therapy.
Drugs for administration
The effectiveness of the procedure depends not only on the qualifications of the specialist who performs it, but also on the quality of the drugs injected into the vein. Despite the abundance of various thrombolytics, not all drugs are equally effective. There are several main groups of medications most often used in thrombolytic therapy .
- A quick positive result can be achieved by using the drug “Prourokinase” during the procedure. However, this medication is not suitable for those patients who have poor blood clotting or are at risk of cerebral hemorrhage.
- The safest and at the same time no less effective and efficient are the drugs “Alteplase” or “Actilyse” - they can alleviate the patient’s condition in a short time. Can be used 5-6 hours after the onset of the first symptoms of an ischemic stroke. However, treatment with these medications requires the administration of heparin.
- New generation drugs Anistreplase, Tenecteplase and Metalise do not require the use of heparin after administration, which greatly simplifies the patient’s treatment process. Moreover, as a result of intravenous administration of the drug, the likelihood of developing allergic reactions is minimized.
- The old generation drug “Streptokinase” is used very rarely. It is the simplest and cheapest among available analogues, and at the same time the medicine has a powerful thrombolytic effect. It can cause serious allergic reactions and provoke the development of hematomas, so “Streptokinase” is used in rare cases and not more than once.
- The drug "Urokinase" is a relatively new drug with a powerful effect. Survival rates are significantly higher than those of analogues (at least fifteen percent). However, the treatment of ischemic stroke with Urokinase requires the use of heparin.
The listed drugs contain mainly natural ingredients. However, regardless of the composition and therapeutic effect, using them independently to eliminate signs of a brain stroke is strictly prohibited. Thrombolytic medications have many contraindications and side effects, which the doctor must take into account before administering the drug intravenously.
Procedure for medical workers
Today, thrombolysis is often practiced for myocardial infarction at the prehospital stage. A drug such as Tenecteplase is best suited for this. It differs from other direct tissue plasminogen activators in its low likelihood of complications, as well as ease of use. "Tenectoplase" is administered intravenously.
Alteplase is also sometimes used for thrombolysis of myocardial infarction at the prehospital level. Before using it, the patient is administered 5000 units of heparin. Then 15 ml of Alteplase is administered intravenously as a bolus. After this, the patient is injected with 0.75 ml of the drug for each kilogram of the patient’s weight over 30 minutes. In this case, the patient is constantly injected with heparin.
"Streptokinase" is recommended to be administered only in a hospital setting. When using this drug, thrombolysis for myocardial infarction is performed in the intensive care unit. The patient is given an intravenous drip of 1,500,000 units of the drug diluted in 100 ml of saline over 0.5-1 hour. In the case of this medication, heparin in a volume of 5000 units is also used before its administration. Subsequently, heparin is used no less than 4 hours after the end of the Streptokinase infusion.
Each form of the thrombolysis protocol for myocardial infarction indicates that this procedure should be performed no later than 12 hours after the onset of the first symptoms of the disease. After thrombolysis therapy, it is necessary to transport the patient to a specialized hospital within 12 hours for the purpose of stenting or balloon angioplasty. Compliance with this procedure significantly increases the patient’s chances of a positive outcome of the disease.
Kinds
Depending on the timing of thrombolysis, the procedure may be:
- selective;
- non-selective.
In the first case, the drugs are administered during the first six hours from the onset of acute circulatory disorders. The main feature of the non-selective technique is the implementation of resuscitation measures during the first three hours.
Depending on the method of drug administration, thrombolysis occurs:
- local. If an examination was carried out in a hospital setting using equipment for intravascular administration, diluting agents are brought as close as possible to the affected area;
- systemic. It is used when there is no information about the location of the blood clot that caused the myocardial infarction. The drugs are administered in the usual way into a vein.
What should the patient do?
Myocardial infarction usually develops in cases where the patient already has another cardiovascular pathology. Most often, this disease is characterized by severe pain in the chest area, accompanied by radiation to the left shoulder, hand, shoulder blade, abdomen or neck, as well as severe weakness. If these symptoms occur, the patient is recommended to call an ambulance, then measure blood pressure and, if its level is at least 120/80 mm. rt. Art. take a nitroglycerin tablet. If after 5 minutes the pain has not disappeared, and the emergency medical team has not yet arrived, you need to repeat taking this drug. In addition, it is recommended to take 500 mg of acetylsalicylic acid (aspirin).
Contraindications for performing thrombus lysis
- internal bleeding that occurred in the last two weeks;
- high blood pressure exceeding 200/120 mm Hg. pillar;
- traumatic brain or other injury, surgery in the last two weeks;
- active peptic ulcer;
- suspicion of pericarditis (bleeding in the pericardial region), threat of aortic aneurysm;
- allergy to the drug with which thrombolysis is planned.
- any surgery or head injury that occurred more than two weeks ago;
- hemorrhagic diathesis (tendency to bleeding) as a reaction to thrombolysis;
- diabetes;
- liver or kidney failure;
- malignant tumors;
- presence of active infection;
- use of anticoagulants in the last six months.
What will the health worker do?
In the case of a paramedic or emergency medical technician, these employees must perform the following actions before starting thrombolysis therapy:
- Clarify with the patient the time of onset and nature of the pain syndrome.
- Perform electrocardiography to clarify the diagnosis of “myocardial infarction” and measure blood pressure levels.
- If this diagnosis is made, the patient is given a nitroglycerin or Aspirin tablet (if he has not taken it previously).
- Subsequently, he is transferred in a prone position to an ambulance.
- Already during transportation to the hospital, the effect of taking nitroglycerin is assessed (5 minutes).
- The patient is also given 5000 units of heparin, at least 40 mg of statins (Atorvastatin, Rosuvastatin, Lovastatin) and drugs from the group of beta-blockers (Metoprolol, Bisoprolol, Carvedilol) and ACE inhibitors ( "Enalapril", "Lisinopril", "Perindopril", "Ramipril") in a dosage that will not reduce the blood pressure level to less than 110/70 mm. rt. Art. and heart rate less than 50 beats/min.
- In the future, the medical professional will clarify the presence of contraindications to thrombolysis. If they are absent, then this procedure begins.
In cases where an inpatient healthcare facility is located near the place where an emergency medical team is called, thrombolysis is often performed in an intensive care unit in order to reduce the likelihood of developing serious complications and most quickly stabilize the patient’s condition if they occur.
In the hospital, thrombolysis therapy is carried out under the constant supervision of a cardiologist/internist and a resuscitator.
After the procedure is completed, doctors stabilize the patient's condition and transfer him to a specialized healthcare facility to perform angioplasty or stenting. After discharge from the hospital, the patient is sent to the outpatient stage of treatment, where he is recommended to take the following medications:
These medications significantly reduce the likelihood of developing recurrent myocardial infarctions. Subsequently, if the patient’s condition is satisfactory, as well as the presence of sufficient recovery potential (the patient is not too old, is able to move, is available for productive contact), he is sent for rehabilitation in order to restore normal functioning. In cases where we are talking about young people, they are often sent to a rehabilitation course immediately after the inpatient stage of treatment.
Methods for dissolving a blood clot
To restore blood circulation in a blocked vessel, two methods are used: intravenous injection in the traditional way or local injection directly into the vessel in which the blood clot is located. There are studies showing that both methods are quite effective in the first 6 hours from the moment of the attack, but the maximum positive results of thrombolysis are observed before the end of the third hour.
It is easiest to dissolve a blood clot in a vein, therefore, with pulmonary embolism (carrying venous blood), smaller doses of enzymes are needed than with atherosclerotic lesions (myocardial or cerebral infarction). It should be taken into account that the dissolution of a blood clot in the deep vein of the lower extremities is dangerous due to its movement to the vessels of the lungs.
With systemic thrombolysis (intravenous administration of medication in a drip) there is a drawback - the risk of bleeding. This is caused by a high dose of the drug, which also increases the risk of unwanted effects.
But it also has an advantage - thrombosis is almost never isolated, so clots from other localizations also undergo dissolution.
With local (selective) administration of enzymes, radiological monitoring of the catheter's progress to the site of blockage is required. This allows the thrombolytic drug to be accurately delivered to the area of impaired blood flow and a lower dose to be applied. It can only be carried out in specialized institutions by doctors skilled in intravascular techniques. It can be effective at a later date (6 - 12 hours) than the systemic one.
Forecast
If the drug dosages are observed, thrombolysis for myocardial infarction is successful in the vast majority of cases. Even with the use of streptokinase, the number of serious complications does not exceed 2%. These performance indicators are relevant in cases where all recommendations for thrombolysis in myocardial infarction are followed.
Despite this procedure, the patient’s further quality of life will largely depend on the completeness and timeliness of other therapeutic and rehabilitation measures. After thrombolysis, patients are recommended to undergo treatment in cardiology departments with possible angioplasty or stenting. Rehabilitation includes physical therapy courses, scheduling of necessary physical activity, as well as regular medications.
How is the effectiveness of therapy assessed?
Criteria for assessing the effectiveness of the thrombolysis procedure:
- Clinical picture: the intensity of the pain syndrome decreases, reperfusion arrhythmias develop.
- Electrocardiogram data: a rapid fall in the ST segment, the appearance of a negative T wave.
- Results of laboratory tests: the activity of CPK (creatine phosphokinase) and its forms decreases, the level of fibrinogen decreases, and thrombin time increases.
- Angiography indicators: the study determines the patency of the heart vessels.
The effectiveness of thrombolytic therapy depends on many different factors, such as:
- Time to start treatment.
- Administration mode.
- The rate of restoration of arterial patency.
- Qualification of specialists conducting treatment.
- Preventive measures to prevent the development of complications.
Features of organizing thrombolysis in a hospital
Drugs that destroy blood clots are most effective within the first 3 hours after an attack. It is permissible to administer them within 12 hours from the moment the first symptoms of a heart attack appear. But if you do this later, the procedure will be ineffective. Therefore, patients receive their first injections of drugs in the ambulance. But these requirements are relevant for patients with myocardial infarction.
Patients admitted with acute cerebral circulatory disorders can undergo this therapy after ischemia has been established. To do this, they must be examined using ultrasound, x-ray or tomograph. The patient must be taken to the hospital very quickly, because... every second is important. The decision to use artificial thrombolysis to improve the patient’s condition is made by the doctor after reviewing the examination results. In case of stroke, this technique allows:
- reduce the time patients stay in hospital by 3-4 days;
- helps to avoid many complications;
- allows 60% of patients to maintain full working capacity;
- allows you to speed up the rehabilitation of patients.
The procedure is most effective in the state before an attack. Then you can avoid almost all complications associated with heart attacks.
Indications for thrombolysis
Indications for thrombolysis
(elderly age is not a contraindication): •
the ECG
shows a rise in the ST interval of more than 1 mm in two or more adjacent leads (if anterior MI is suspected) or in 2 of 3 limb leads II, III, avF (if an inferior MI is suspected ), or the presence of LBBB (probably when subtotal coronary artery occlusion progresses to total), or idioventricular rhythm,
• first 6 hours of myocardial infarction
. But if pain persists, ST segment elevation and the absence of the Q wave (when the myocardium is still alive), the first 12 hours are also “suitable”, if the MI has not ended and there is a “mosaic” clinical picture. The decision to perform thrombolysis after 12 hours is made on the basis of clinical pictures, anamnesis and ECG
Carrying out thrombolysis
for ACS without persistent ST segment elevation (or with T wave inversion, or no changes on the ECG) is not indicated