In cardiology, pharmaceutical organic nitrates, whose more precise name is nitrovasodilators, are used to treat patients with angina pectoris, coronary artery disease, and acute coronary syndrome.
Short-acting nitrate is the best drug for self-relief of angina attacks
These heart medications today come in many forms: sublingual tablets, cheek patches, oral capsules, chewable lozenges, aerosols, sprays, ointments, skin patches, intravenous solutions.
The doctor decides which drug (active substance, duration of action, form) to prescribe to the patient. At the same time, he takes into account the diagnosis, stage of the disease, purpose of use, contraindications and side effects of nitrates.
Description, mechanism of action of nitrates
Nitrates (nitrovasodilators) are medications that can dilate the heart arteries, stopping an attack of ischemic pain.
Solutions of organic substances of this type began to be used in the treatment of angina pectoris at the end of the 19th century, and already at the beginning of the 20th century, medical practice received the first capsule preparations, tablets under the tongue. The disadvantage of the drugs was their short-term antianginal effect. At the end of the 70s of the last century, it was possible to synthesize long-acting nitrates for the treatment of angina pectoris, thereby solving the existing problem.
The mechanism of action of nitrates consists of relieving vasospasm and relieving pain. The essence is relaxation of the smooth muscles of the vascular wall, increasing the lumen of the coronary arteries, delivering the necessary nutrition and oxygen to the myocardium. For this, nitrates are capable of:
- stimulate the work of collaterals, through which an additional volume of nutrients is delivered to the heart, preventing the risk of hypoxia and ischemia;
- exhibit a vasodilator effect, reducing peripheral blood resistance, thereby reducing the load on the heart muscle;
- expand the veins, which reduces venous blood flow, compensatingly improving blood flow in the coronaries, reducing the load on the ventricles, and improving the contractility of the cardiomuscle.
When nitrates enter the human body, they instantly release the NO group (nitric oxide), which stimulates the synthesis of a special enzyme - guanylate cyclase, causing an increase in the concentration of guanosine monophosphate - a nucleotide that is part of RNA.
The accumulation of this substance in vascular cells leads to relaxation of smooth muscles wherever they are present: coronary arteries, bronchi, urinary system, digestion. At the same time, nitrates block the connection between the periphery and the brain: the sympathetic system loses control over the blood vessels and heart, and coronary spasm becomes impossible.
The analgesic effect is supported by hemodynamic unloading of the myocardium, which reduces the heart's need for oxygen. The wide lumen of the arteries, combined with minimization of resistance during cardiac contraction, facilitates the work of the myocardium. The expansion of the veins ensures that the return of venous blood to the heart is limited.
The use of nitrates balances the electrolyte composition of the blood, stimulates respiratory enzymes, improves the condition of the cardiac conduction system, preventing arrhythmias. In addition, the drugs reduce pressure in the pulmonary circulation, relieving left ventricular failure. Medicines can reduce the adhesion of red blood cells, improving blood flow, allowing the heart muscle to more easily cope with unusual or excessive load.
Tolerance and sensitivity to nitrates in patients is strictly individual. For some, a tablet is enough to solve the problems that have arisen, which does not cause any discomfort. Others suffer severe attacks of headaches after taking a minimal dose of nitrates, which makes taking the drugs problematic and requires searching for an alternative.
The duration of the anginal effect ranges from an hour to eight. Therefore, the correct, leisurely selection of the right medicine by the doctor for each patient is very important.
A little history
Nitroglycerin has been used to relieve angina attacks since the end of the 19th century.
Organic nitrates were first used to relieve pain due to angina back in 1879. Dr. Murrell published the results of exposure to a 1% alcohol solution of nitroglycerin (glycerol trinitrate) in the Lancet journal. He first “tried” this drug on himself and then on his patients. The results of antianginal effects were positive.
In 1925, capsules with Nitroglycerin entered the practice of cardiologists, and a little later a liquid alcohol solution and tablets for administration under the tongue appeared. However, cardiologists were not satisfied with the short-term effect of this drug, and pharmacological studies aimed at finding similar long-acting substances continued. After the 70s, the first such drug was created based on isosorbide dinitrate, and a little later a new nitrate-containing product appeared - isosorbide mononitrate.
All these active components have the same mechanism of action; it consists of a vasodilator and antianginal component. Thanks to the effects of organic nitrates, vascular smooth muscles relax, coronary vessels dilate, and more blood and oxygen are delivered to the myocardium. As a result, the hemodynamic load on the heart and the oxygen demand of the heart muscle are reduced.
Classification
There are several approaches to classifying nitrates. All drugs are divided according to the active substance into three groups:
- Nitroglycerin group.
- Isosorbide mono- and dinitrate.
- Nitro-like agents.
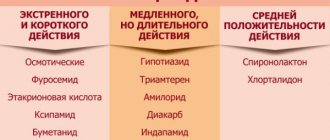
According to the duration of the analgesic effect on:
- short, the duration of pain relief is up to 1 hour;
- medium - from one to six hours;
- prolonged - up to a day.
According to pharmacological forms:
- point of application – oral cavity: sublingual tablets, liquid capsules, wafers, aerosols;
- oral, entering the body through the mouth: tablets and capsules;
- ampoule solutions: for intravenous or intramuscular injections.
Classes of angina pectoris and features of taking nitrates
The principles of therapy depend on what functional class of angina was identified in the patient:
- In the case of the first class of pathology, it is recommended to take the drug before the expected load. Depending on the type of nitrates taken, this should be done either an hour or 5 minutes before activity.
- The second class of angina also requires taking the drug before exercise. If attacks recur frequently, prolonged forms are indicated.
- For third class angina, long-acting medications are taken (up to 12 hours).
- For fourth class pathology, medications are taken with a duration of up to 16 hours.
After the patient feels pain in the chest area, he should take a sitting position and put a tablet under his tongue. If the attack begins while the patient is in a supine position, he needs to sit down: this way the attack will pass faster.
Indications for use
The main indication for the use of nitrates is vasospasm of the cardiac arteries, ischemia, and myocardial hypoxia. Relatively recently, medications were used for differential diagnostic purposes: with the help of Nitroglycerin, myocardial infarction was distinguished from angina pectoris (an attack of cardialgia was stopped by nitrates, a developing heart attack was not). Today, there are more accurate instrumental and laboratory methods for diagnosing AMI, but when providing first aid to heart patients, there is still no better alternative than Nitroglycerin or its analogues.
Nitrates are recommended for use when:
- myocardial ischemia of any origin (for the prevention of an attack of angina - before the planned exercise, for treatment - first aid);
- left ventricular failure;
- hypertensive crisis;
- acute heart failure (prevention or relief of pulmonary edema);
- CHF;
- arrhythmias due to deterioration of the trophism of the heart muscle;
- complex treatment or prevention of thrombosis, thrombophlebitis.
Medications
Medical substances close to organic nitrates (sodium nitroprusside, nitrites, molsidomine) also have a nitroxidergic effect.
They have well-known differences in pharmacokinetic parameters and indications for use (nitroglycerin is used mainly to eliminate angina attacks, other medications are used to prevent their development). Adverse reactions of individual medications are mainly due to the mechanism of action common to the entire category of these drugs, and therefore are very similar.
List of drugs with different durations of action
Nitrates are available in different dosage forms: from tablets, injections to transdermal or buccal strips. The duration of action directly depends on the form of the drug:
- sublingual tablets, capsules, granules (the expiration date expires two months from the moment the bottle is opened) or aerosols (the can contains freon, an environmentally hazardous substance, but there are no significant advantages over tablets) are intended to quickly relieve an attack of angina;
- tablets, capsules for oral administration, solutions for injections - used in the treatment regimen for coronary heart disease and heart failure.
Nitrates with an effect of up to an hour
These include drugs based on nitroglycerin, isosorbide mononitrate and dinitrate.
Nitroglycerin begins to act 60 seconds after administration, the peak occurs in the fourth minute of administration, and the effect ends after half an hour. That is why the drug can be taken a couple more times with an interval of 5 minutes.
Infusions of nitroglycerin nitrates are recommended for unstable angina and AMI. Method of administration: dropper with gradually increasing infusion rate. Monitoring of systolic pressure (at least 90 units) is mandatory. The pain goes away in a couple of minutes. Maintenance administration is continued for up to 10 hours.
Nitrates with this effect for preventing an attack of angina or relieving it include:
- Nitroglycerin - sublingual tablets (16 rubles), capsules (10 rubles) and aerosols (preferred for dry mouth - 113 rubles);
- Perlinganite – sublingual tablets (729 rubles);
- Carniland – drops under the tongue (118 rubles);
- Nitrocor – sublingual tablets (57 rubles);
- Nitromint - spray under the tongue (146 rubles);
- Nitrospray - nitrate in aerosol (103 rubles);
- Isoket is a peripheral vasodilator with a predominant effect on venous vessels (909 rubles);
- Isosorbide dinitrate – tablets under the tongue (29 rubles);
- Isosorbide mononitrate – tablets – 52 rubles, capsules – 102 rubles.
Nitrovasodilators lasting up to 6 hours
Nitrates of this group are represented by peripheral vasodilators, affecting mainly the veins. The drugs demonstrate an analgesic and antiangiospastic effect due to:
- reducing pressure in the pulmonary circulation;
- relief of hypoxia;
- redistribution of coronary blood flow, expansion of the coronaries themselves;
- increasing tolerance to physical activity;
- reducing the load on the left ventricle;
- relaxation of smooth muscles;
- balancing electrolytes;
Once ingested, part of the drug dose begins to act within 10 minutes, while the other is absorbed into the bloodstream slowly, ensuring that the therapeutic effect of nitrates is extended for another 6 hours.
Such medications are appropriate only for the prevention of angina attacks. These are retard drugs based on nitroglycerin, isosorbide dinitrate and isosorbide mononitrate for oral administration, which are available in different forms and dosages, which makes it easy to adjust the amount of the drug per dose. An example would be:
- Nitroglycerin retard (Glycerol trinitrate) – 80 rubles;
- Isoket retard – 394 rubles;
- Nitrodurate – 140 rubles;
- Nitrosorbitol – 40 rubles;
- Nitrogranulong – 60 rubles.
In addition, there are buccal plates or tablet applicators. These nitrates are intended to relieve angina pain or prevent recurrent attacks over the next 5 hours. Nitrates of this group have the highest bioavailability. These include:
- Trinitrolong – 55 rubles;
- Sustabukkal – 75 rubles;
- Dinitrosorbilong - provides a therapeutic effect for more than 10 hours (66 rubles):
- Dikor Long – 70 rubles.
Nitrates with effectiveness up to 24 hours
Long-acting nitrates - transdermal patches and sprays for relieving angina attacks begin to act in half an hour, and end in a day. The drugs are not very popular among patients due to local irritating effects on the skin, rapid addiction and high cost. This includes:
- Minitron (Nitrocor) – 50 rubles;
- Nitroderm – 1860 rubles;
- Nitrodur – 330 rubles;
- Nitro-lor – 41 rubles;
- Nitromint – 132 rubles;
- Isodinite – 100 rubles
Medication dosages
Nitroglycerin is used as follows:
- capsules with a 1% oil solution in a dose of 0.001 and 0.0005 g;
- tablets 0.0005 g;
- aerosol for sublingual use - 0.0004 g;
- alcohol solution - 1-2 drops per sugar.
To prevent attacks of angina pectoris, long-acting tablets for oral administration are used - “Nitrong”, “Nitrogranu-long”, “Sustak forte”. The list of organic nitrates is quite extensive. After taking these medications, the effect of the main element begins after 120 minutes and lasts about 6 hours. These products are also used according to the transdermal therapeutic system - special patches (“Deponit”), which are glued to the skin for 12 hours (the patch releases 0.0005 g of the substance per day).
Isosorbide dinitrate is administered sublingually, its effect develops after 3-5 minutes, when administered orally - after 15-30 minutes. The dosage is one tablet at a time, further use is determined by the treatment regimen established by a specialist. Despite the widespread use of this drug in modern medical practice, its use is best agreed with a doctor, due to the pronounced clinical effect and possible adverse reactions.
Contraindications
Nitrate intake is limited in many cases. First of all, these are common pathological conditions that require emergency intervention and pose a risk to life. For example:
- vascular collapse with a drop in blood pressure below 90 mm Hg. Art.;
- cardiogenic shock;
- a sharp drop in blood pressure;
- attack of myocardial ischemia;
- head injury;
- high intracranial pressure;
- ONMK;
- angle-closure glaucoma;
- anemia;
- pulmonary edema;
- uncontrolled arrhythmia:
- hypersensitivity to drugs.
Nitrates are recommended with caution to patients diagnosed with cerebral atherosclerosis. During pregnancy, drugs in this group can cause intrauterine fetal death. Breastfeeding involves giving up nitrates or transferring the baby to artificial formulas, since, when penetrating into breast milk, the drugs cause hemodynamic disorders in the baby, methemoglobinemia.
Expert advice
In order to receive a course of nitrates, you need to contact a competent specialist. As a rule, this is an ordinary therapist or cardiologist. After prescribing the drug, further monitoring of the patient's condition is required. It allows you to identify side effects in time and adjust the dose or change the drug. Several factors may indicate the effectiveness of treatment:
- The patient tolerates physical activity better.
- The number of angina attacks decreases.
- Systolic blood pressure decreases to 15-25 mmHg. Art. at rest.
In some cases, to monitor the effectiveness of treatment, the patient is subjected to slight physical activity and observed how the body copes with it. This method clearly shows how effective the treatment is.
Before taking the medicine, experts recommend carefully reading the instructions for use and understanding the mechanism of action of nitrates for angina before starting their use. Exceeding the dose can have a detrimental effect on health, as can abrupt withdrawal of the drug. The dosage of the medication should be reduced gradually to give the body time to get used to the changes. You can get all the recommendations from your doctor, because it is extremely important that the dosage of the medicine and the duration of the drug are selected correctly, taking into account the severity of the disease and the patient’s condition.
Side effects
Side effects when using nitrates are also not uncommon. They can be conditionally divided into two groups: frequently occurring and observed in exceptional cases. The first group includes:
- vascular pulsations, migraine;
- hypotension, VSD;
- orthostatic collapse;
- cardiopalmus;
- slowing of the pulse during intravenous infusions;
- redness of the face;
- rapid addiction to drugs;
- withdrawal syndrome;
- symptoms of intoxication;
- retrosternal discomfort;
- hypoxia with cyanosis of the nasolabial triangle (life-threatening).
Rare side effects from taking nitrates include:
- high intraocular pressure;
- skin rashes;
- dyspepsia;
- methemoglobinemia.
Tolerance and withdrawal syndrome
Tolerance syndrome is becoming the scourge of modern conservative therapy. Pharmacological drugs that initially have an excellent therapeutic effect, over time, practically cease to produce results from their use. This happens, for example, when using antibiotics because microbes become accustomed to active antibacterial substances. Something similar happens to the coronary arteries: the vessels stop dilating in response to the use of nitrates.
Pharmacologists have found a way out of this situation. Scientists have proposed creating a so-called “nitrate-free window.” This is a period of time when there are no nitrates in the bloodstream. The body has time to “cheer up”. For example, instead of taking the drug four times, make it three times, use more retard, prolonged forms (today the base in the form of isosorbide-5-mononitrate has already been synthesized).
The “nitrate-free window”, when used excessively, also has a downside. Frequent breaks in taking nitrates entail withdrawal syndrome. For example, Nitroglycerin and its derivatives are widely used for preventive purposes. But this is nothing more than an intermittent method of introducing the drug into the body. Nitrates are taken only before physical activity. Moreover, long-acting drugs are used.
The body has time to get used to them, and the sudden withdrawal of nitrate protection provokes chest discomfort with an unpredictable development of the attack. Therefore, for the purpose of prevention, nitrates are prescribed only to those patients in whom an angina attack is inevitable without the use of medications. Single-dose medications are selected.
How to avoid addiction to nitrates
So far, the mechanism of reducing tolerance to organic nitrates has not been fully studied, and experts put forward only speculative reasons for the occurrence of such a side effect. In addition, the development of addiction varies among patients. For example, taking isosorbide dinitrate for a month is accompanied by a complete loss of the antianginal effect in approximately 10-15% of patients, in 60-70% this effect is significantly reduced, and in 10-15% it remains the same. According to the observations of specialists, a decrease in tolerance to nitrate-containing products most often occurs when using transdermal forms, and much less often when using buccal tablets and plates.
To reduce or eliminate the addictive effect, it is recommended to take organic nitrates with the obligatory observance of a period free from taking these drugs. According to experts, for this it is enough to observe an 8-12-hour “nitrate-free” interval.
In addition, if possible, you should take breaks from taking nitrate-containing products. This interval can be 1-2 weeks. If it is impossible to completely cancel nitrates during this period, the usual drug can be replaced with Corinfar or Sidnopharm (Corvaton).
Nitrates for cardiac ischemia
The options for using nitrates for ischemic heart disease are different. Stable angina, for example, is correlated with functional classes. With 1-2 FC, nitrates are taken only before physical activity; there is no need to use complex forms. FC III-IV suggest the prescription of prolonged medications (Cardiket-retard, twice a day). For nocturnal symptoms, isosorbide-5-mononitrate (40 mg twice a day) is indicated.
Heart attack or unstable angina requires great caution. Drip administration of nitrates is used under constant monitoring of blood pressure levels. The activity of nitrovasodilators is enhanced in the presence of calcium antagonists (Verapamil, Diltiazem, Norvasc), beta blockers (Betalok, Propranolol, Obzidan), antiangitensin inhibitors (Losartan, Telmisartan, Rasilez).
Prescription of drugs depending on the functional class of angina
In patients with angina pectoris of functional class 1-2, nitrates should be taken intermittently, before situations that may cause an attack. This is not difficult, since with these types of pathologies, attacks occur predictably, at certain times and days and with specific types of physical activity.
For the first and second classes of angina pectoris, nitrate-containing drugs of short and moderately long action are indicated.
For patients whose angina is more severe, nitrates are prescribed in such a way as to ensure the effect throughout the day. This is due to the fact that with such forms of pathology, attacks occur even at rest. To achieve this goal, either regular-duration medications are prescribed 3-4 times a day or long-acting medications 1-2 times a day.
Interaction with other drugs (possibility of combination treatment)
The prevalence of coronary artery disease, angina pectoris, rest, and other forms of cardiovascular pathology automatically implies the inclusion of nitrates in a complex therapy or combination treatment regimen. In this case, one should take into account the ability of other drugs to lower blood pressure, which is undesirable when combined with nitrates. Drugs that can cause hypotension include:
- drugs that stimulate potency (Sildenafil, Viagra, BestJack);
- derivatives of barbituric acid (Phenobarbital, Barbital, Hexobarbital), there are no freely available drugs;
- opioids (Nalorphine, Pentazocine, Buprenorphine);
- tricyclic antidepressants (TAC) – Azafen, Amitriptyline, Fluoracisine;
- antihypertensive drugs (Renitek, Enalapril, Cardosal, Lisinopril, Quinapril).
Ethyl alcohol has a similar effect. A combination of nitrates with histamine, angiotensin, carbacholine, phenylephrine, atropine (M-cholinergic blockers), central nervous system stimulants, and hormones can be negative.
Literature
- Mazur N.A. The role of nitrates in the treatment of cardiac patients in accordance with the principles of evidence-based medicine and recommendations for their practical use. Cardiology, 2005.
- Lupanov V.P. Nitrates. In the book:. Rational pharmacotherapy of cardiovascular diseases: a guide for practitioners. Compendium Under the general ed. E.I. Chazova, Yu.A. Karpova. 2nd ed. corr. and additional M.: Litterra, 2020.
- Kryzhanovsky S.A., Vititnova M.B. Medicines for the treatment of coronary heart disease (basic, clinical and evidence-based pharmacology). Lecture 2, part 1. Organic nitrates and their place in the pharmacotherapy of coronary heart disease. Therapist, 2011
- Thadani U. Challenges with nitrate therapy and nitrate tolerance: prevalence, prevention, and clinical relevance journal. Amer J Cardiovasc Drugs, 2014.
- Munzel T, Steven S, Daiber A. Organic nitrates: update on mechanisms underlying vasodilation, tolerance and endothelial dysfunction. Vascul Pharmacol, 2014
Lyudmila Zhavoronkova
Higher medical education. 30 years of working experience in practical medicine. More about the author
All articles by the author
Nitrates in the practice of treating myocardial infarction
Nitroglycerin (NG), belonging to the group of organic nitrates containing NO3 in the compound, the chemical name of which is glycerol trinitrate, is one of the most long-used drugs in cardiological practice. In 1847, Ascanio Sobrero first created NG for industrial purposes (manufacturing an explosive - dynamite), and 6 years later - in 1853, Harring first used it to treat “angina pectoris” - the clinical equivalent of angina attacks. Since 1879, NG, as a first-line drug, has been widely used in the relief of anginal attacks. And only 120 years later, after studying the bio-pharmacodynamics of nitrates and the discovery of endothelium-dependent relaxation factor (EDFR), organic nitrates were accepted as the basis for the treatment of diseases associated with coronary pathology - IHD. Organic nitrates mimic the physiological effects of EGFR, which was identified in 1998 as nitric oxide - NO. The biological importance of the discovery of ESFR was assessed by the awarding of the Nobel Prize to scientists: Robert Furchgott, Luis Ignarro, Ferid Murad
.
Currently, organic nitrates are the most common agents in the treatment of cardiovascular diseases, in particular in AMI.
Organic nitrates are donors of exogenous NO, which is identical in its physiological effect to endogenous NO. They become active after a number of metabolic transformations, as a result of which nitric oxide is formed - a substance similar to the structure and function of EGFR. In endothelial and smooth muscle cells, organic nitrates release nitric oxide through biochemical transformations. It has been shown that these cells are capable of metabolizing NG into glyceryl dinitrate, followed by the release of nitric oxide. It is assumed that nitrates interact with intracellular vascular receptors that contain one or more reduced SH groups. This interaction is necessary for the pharmacological transformation of nitrates. In this case, nitrates oxidize reduced SH groups to disulfides, which are able to re-interact with nitrates.
The proposed scheme of metabolic transformations of organic nitrates has now been sufficiently studied and looks in the following sequence: initially (presystemic metabolism), organic trinitrates (NO3), passing through the liver, are converted into dinitrates - nitrogen dioxide (NO2), in particular isosorbide-2-dinitrate - “first pass effect” (“first – pass – effect”); then, organic dinitrates in endothelial and smooth muscle cells, under the action of enzymes located on the outer side of the cell membrane, are transformed into mononitrates through the intermediate formation of nitrosotyl (R-SNO), which serves as an intermediary for the formation of NO. In this enzymatic transformation, hydrogen sulfide radicals (SH) serve as cofactors. The resulting NO stimulates soluble guanylate cyclase in smooth muscle cells with an increase in the synthesis of guanosine monophosphate, which is accompanied by a decrease in the cytosolic concentration of Ca++ and, as a result, relaxation of muscle cells develops. In accordance with the biological law - the mechanism of uniformity of action, similar biochemical events take place in platelets, which leads to a decrease in their functional activity (“calming”) (Fig. 1).
Rice. 1.
Diagram of the physiological effects of endogenous nitric oxide (NO) with an intact (A) and nitrates with a damaged endothelial layer (B) of the vascular wall
Vascular endothelial cells (in particular coronary arteries) perform an important hemodynamic regulatory function. They have anti-inflammatory and anticoagulant properties. It has been established that the main mediator that allows these functions to be carried out is nitric oxide, produced by the endothelial cell with the help of the enzyme nitric oxide synthase in response to stimulating signals - serotonin, thromboxanes, catecholamines, flow-dependent shifts of endothelial cells, etc. Nitric oxide has a vasodilating effect and at the same time acts as a powerful inhibitor of platelet aggregation and adhesion on the inner surface of the vascular wall. Nitric oxide has the ability to block the expression of genes responsible for the formation of adhesion molecules - ICAM-I, VCAM-I and 3-selectin, and inhibits the synthesis of monocyte chemottractant protein (MCP-I). Thus, it prevents the penetration of inflammatory cells and reduces the diffusion of low-density lipoproteins into the vascular intima. In addition, nitric oxide has anti-inflammatory and antioxidant effects by interacting with oxygen free radicals.
A decrease in the bioavailability of nitric oxide can occur both as a result of a decrease in its synthesis and as a result of an increase in its consumption (“EZFR - consumption pathology”). In atherosclerosis under the influence of risk factors, both ways of reducing the bioavailability of nitric oxide can occur, manifesting themselves separately or in combination. Nitric oxide synthesis is significantly reduced in inflammatory or atherosclerotic endothelial damage, and these disorders are the main manifestations of endothelial dysfunction.
Many risk factors for atherosclerosis worsen endothelial function and reduce the total bioavailability of nitric oxide. For example, hyperlipidemia reduces the bioavailability of nitric oxide by impairing flow-dependent arterial dilatation, and statin use increases the bioavailability of nitric oxide.
Diabetes mellitus is accompanied by dysfunction of the endothelium, which is manifested by a decrease in the synthesis of nitric oxide. Oxidative stress, which occurs in various pathological conditions, is accompanied by an increase in oxidized low-density lipoproteins and oxidative inactivation of nitric oxide. Arterial hypertension and smoking also lead to endothelial dysfunction and decreased bioavailability of nitric oxide.
Currently, leading experts in the field of cardiological pharmacology postulate that the mechanism of action of organic nitrates is explained by its simulating endothelial relaxation factor (NO) and does not depend on the functional state of the endothelium. The need for such “replacement” therapy arises in many diseases of the cardiovascular system that are based on endothelial dysfunction, i.e. the presence of an imbalance between intravascular constrictor and relaxing factors produced by the endothelium.
The anti-ischemic effect of organic nitrates is due to the summation of two mechanisms of action: NO-replacement (with endothelial dysfunction) and vasodilatory hemodynamic effects (reduction of “pre- and afterloads”).
As stated earlier, IHD is a discrepancy between the magnitude of coronary blood flow and the level of myocardial oxygen consumption (PM02). Normally, the value of coronary blood flow is slightly higher than the level of oxygen consumption by the myocardium - the heart is in a state of “superperfusion”. An imbalance between oxygen delivery and the intensity of its consumption by the myocardium can occur either with an excessive increase in oxygen consumption (intensive work of the heart as a pump), exceeding the delivery capacity, or with a significant decrease in the volume of oxygen delivery (occlusion of the coronary arteries, anemia) with a normal level of oxygen consumption (resting state). ).
The level of PMO2 depends on heart rate, contractile state of the myocardium and intramyocardial tension. Heart rate has a double effect on the value of PMO2 through an increase in rhythm (increase in work) and a decrease in diastole time, during which blood supply to the left ventricular myocardium occurs (O2 delivery). An increase in the contractile state of the myocardium - the speed and force of contraction of the cardiomyocyte, developed in response to an increase in total vascular peripheral resistance (TPVR) - “afterload”, increases the consumption of ATP, the product of oxidative phosphorylation in mitochondria after oxygen enters the cell. Intramyocardial tension, determined by the Laplace formula (T=P R/2), is also involved in the regulation of O2 consumption and depends on the end-diastolic pressure in the cavity of the left ventricle and the end-diastolic volume - blood flow to the heart (“preload”).
The volume of coronary blood flow, according to the Poiseuille formula - Qcor = ΔP/Rcor, is regulated by the pressure gradient (between the mouth of the coronary arteries and intramyocardial tension during diastole - AR) and the resistance of the coronary vessels - Rcor.
The main effect of NG is the relaxation of the smooth muscles of the vascular wall, mainly the venous bed, since the capacity of the venous bed is 20 times greater than the arterial bed. The vasodilatory effect of organic nitrates leads to a significant reduction in pre- and afterload of the ventricles of the heart, which reduces filling pressure, intramyocardial tension and improves blood circulation in the subendocardial and intramural areas in diastole, with a redistribution of blood supply in favor of ischemic areas.
Organic nitrates have a vasodilating effect on the coronary vessels, especially when the function of their endothelium is impaired, in particular in patients with atherosclerosis, when initially there is a violation of vasomotor tone. Arteries affected by atherosclerosis (altered endothelium) are characterized by hypersensitivity to vasoconstrictor stimuli (thromboxanes, catecholamines). The improvement of coronary blood flow is also facilitated by the antiplatelet activity of organic nitrates, which is similar to the inhibitory effect of endogenous NO on platelet aggregation and adhesion.
Currently, a great similarity has been shown between the effects of nitrates and EGFR, since it is endogenous NO. From these positions, the effect of nitrates can be called “substitution”, those similar to EZRF, and organic nitrates themselves “exogenous EZRF”.
In patients with coronary artery disease and angina, organic nitrates have the following beneficial pharmacological effects:
1 - reduce the consumption of PMO2 (reduce pre- and afterload due to the expansion of systemic veins and arteries);
2-increase and redistribute coronary blood flow in favor of the ischemic myocardium (by reducing intramyocardial tension and relieving ischemic contracture of the myocardium);
3 - partially compensate for the disruption of endothelial dysfunction in the process of NO release by compensating for the lack of EGFR;
4 - improve the rheological properties of blood (increases the mobility of erythrocytes and inhibits the aggregation and adhesive activity of platelets).
Today, as a result of active study of metabolism and mechanism of action, organic nitrates are represented by three groups: nitroglycerin - glycerol trinitrate, isosorbide dinitrate and isosorbide-5-mononitrate (Table 1). The most widely used organic nitrate preparations, nitroglycerin, isosorbitol dinitrate, and isosorbitol 5-mononitrate, differ significantly from each other in pharmacokinetic parameters. Based on the pharmacological characteristics of metabolism, various dosage forms of organic nitrates have been created: solutions for intravenous administration (Perlinganit - nitroglycerin, Isoket 0.1% solution - isosorbide dinitrate), tablets (Efox 20), capsules (Efox Long 50), aerosols for oral use (Isoket), skin and gum patches, ointments.
Table 1.
Pharmacological properties of organic nitrates
| Pharmacological profile | Glycerol trinitrate (nitroglycerin) | Isosorbide dinitrate | Isosorbide-5-mononitrate |
| "First-pass-effect" | Occurs | Occurs | Absent |
| Bioavailability | 50% (sublingual) | 50% (sublingual) 22% (orally) | 100% (inside) |
| Duration of action | 10-30 minutes (sublingual) | 30-60 minutes (sublingual) 180-360 minutes (orally) | 300-380 minutes (orally) |
| Half-life | 2-4 minutes | 30-40 minutes | 240-360 minutes |
| Release form (route of administration) | percutaneously, sublingually, orally, intravenously | sublingually, orally, intravenously | inside |
When prescribing organic nitrates in the practice of treating major cardiovascular diseases, one must be guided by the following provisions:
1 — selection of the optimal drug (ease of administration and effectiveness);
2 — assessment of tolerance to organic nitrates;
3 - exclusion of side effects (individual sensitivity).
The selection of a drug is considered optimal when there are no undesirable effects with successful treatment. Treatment is considered successful when the ischemic attacks are completely or almost completely eliminated and the patient returns to normal social or physical activity, i.e. transfer to functional class I (FC), when pain attacks occur only under significant load.
Drug tolerance is the absence or weakening of the therapeutic effect with a single or regular use of a drug. Tolerance to nitrates, according to various authors, when taken regularly, develops in 60-75% of cases, while a complete lack of therapeutic effect is recorded in 10-15% of cases.
Long-term intake of nitrates depletes the reserves of SH groups in the blood vessels, which can lead to a resistance effect. SH-group donors are methionine (precursor of L-cysteine) and N-acetylcysteine.
There are several hypotheses for the development of nitrate tolerance:
1 - metabolic (depletion of sulfhydryl (SH) groups, inhibition of the conversion of nitrates into nitric oxide, increased activity of cGMP phosphodiesterase;
2 - neurohormonal activation (compensatory activation of constrictor biologically active substances - endothelium-1, renin, angiotensin, catecholamines, thromboxanes, etc.);
3 - oxidative stress (increased content of free radicals - superoxide).
Prevention of the development of tolerance to organic nitrates is possible if the following provisions are observed:
a - selection and dosage of the drug;
b — intermittent administration of nitrates throughout the day;
c - discontinuation of the drug (replacement with other antianginal drugs - beta blockers, calcium antagonist);
d - prescription of “correctors” (SH-group donors, ACE inhibitors and AT receptor blockers, antioxidants).
The low bioavailability of glycerin trinitrate and isosorbide dinitrate when taken orally makes it difficult to select an effective therapeutic dose of these drugs in clinical practice, therefore, in the treatment of stable angina, preference should be given to isosorbide - 5 - mononitrate, the bioavailability of which when taken orally reaches 100%.
The most common side effects of nitrates are headaches and orthostatic hypotension. With intravenous administration of nitroglycerin, methemoglobinemia may develop, which disappears after discontinuation of the drug. In addition, caution should be exercised when using heparin concomitantly, as coadministration may potentiate hypocoagulative effects.
Indications for the use of nitrates are all types of angina pectoris in order to prevent anginal attacks and their complications (ACS, MI), and improve the quality of life. The most commonly used retardated-release drugs, isosorbide-5-mononitrate, are quite effective in preventing painful attacks and silent episodes of myocardial ischemia for 12-19 hours with a single daily dose and can improve LV systolic and diastolic function. Their use makes it possible to reduce the dose and frequency of taking the drug to 1 time per day, and reduce the development of “rebound” syndrome.
Despite the lack of absolute evidence of the effect of nitrates on the survival of patients with unstable angina (ACS), their effectiveness is nevertheless generally accepted. When anginal attacks develop at the prehospital stage, multiple sublingual administration of NG is used. If pain persists and there are no contraindications, NG is administered intravenously with titration of the administered dose until a hemodynamic effect is achieved - a decrease in SBP by 10-20% of the initial value, but not lower than 90 mmHg, and in patients with hypertension - by 20-25% of the initial value . Due to the development of tolerance to NG with intravenous administration lasting more than 24 hours, discrete administration of organic nitrates or an increase in the rate of drug administration is recommended. We must not forget that if the drug is abruptly discontinued, a “rebound” syndrome may develop - the appearance of pain (recurrence of angina), the spread of the ischemic zone, with aggravation of hemodynamic manifestations (increase in blood pressure), especially after IV use of NG.
According to multicenter controlled studies (ISIS-4, GISSI-3), in the treatment of AMI with intravenous NG administration, a decrease in hospital mortality of up to 35% (in the first week) and a good clinical effect in subsequent months were noted. According to a number of authors, intravenous administration of NG solution (Perlingait) or isosorbide dinitrate (Isoket) should be started at a rate of 10-20 mcg/min; if blood pressure is not sufficiently reduced, the dose of the drug is increased by 5-10 mcg/min every 5-10 minutes. The maximum daily dose of nitrates can reach 200 mcg for 2-3 days. This dose provides a significant reduction in pulmonary artery wedge pressure (PAWP) while maintaining a sufficient cardiac output (CI).
The positive effect of nitrates in the first 4-6 hours from the onset of a heart attack is primarily due to the limitation of the necrosis zone and the beneficial effect on coronary blood flow through collateral vessels. It is especially advisable to administer NG intravenously in patients with anterior MI, for whom artificial thrombolysis is contraindicated. Organic nitrates not only effectively eliminate clinical and ECG signs of myocardial ischemia, but also reduce post-infarction LV remodeling. Intravenous infusion of NG is indicated in the first 24-48 hours from the onset of the disease in patients with HF, large anterior MI, hypertension and persistent myocardial ischemia. If angina or left ventricular failure persists (especially with pulmonary congestion, pulmonary edema), longer use of nitrates is necessary. IV administration of nitrates should be used with caution in patients with posterior MI, which is often (in 50% of cases) combined with right ventricular myocardial infarction, since there is a decrease in blood flow to the right side of the heart due to venous dilatation and deposition of blood in the venous channel, can cause severe hypotension due to low cardiac output syndrome on the part of the left ventricle. Contraindications for the use of NG are low blood pressure (SBP J 90 mm Hg) combined with bradycardia (<50 beats per minute) or tachycardia (>110 beats per minute).
Intravenous infusion of NG (Perlinganite) is preferable in the treatment of ACS in patients with unstable hemodynamics, since it has a short duration of action. In all other cases, isosorbide dinitrate (Isoket 0.1% solution) must be used for infusion therapy. The positive clinical effect of intravenous administration of organic nitrates in ACS is due to a decrease in pre- and afterloads, which altogether brings the level of PMO2 into line with Qcor
. In addition to reducing pre- and afterload, nitrates reduce intramyocardial tension through a decrease in filling volume and left ventricular end-diastolic pressure (LVEDP). The improvement in the relaxation ability of the myocardium is caused by the relief of myocardial ischemia by enhancing collateral oxygen delivery and eliminating ischemic contracture. All these mechanisms are well documented when monitoring central hemodynamics before and after titrated intravenous administration of Isoket 0.1% solution under blood pressure control during the treatment of AMI (Fig. 2). Improving the diastolic function of the left ventricular myocardium retrogradely helps to reduce the pulmonary artery wedge pressure and improve the gas exchange function of the lung.
Rice. 2.
Dynamics of pressure in the right and left parts of the heart before and after treatment of a patient with AMI
We observed 57 patients with AMI (4-6 hours from the onset of the disease) aged from 43 to 57 years (51.56±1.7 years) with no history of indications of a previous MI. All patients underwent monitoring of central hemodynamics with registration of pressure in the left and right parts of the heart, pulmonary artery, and aorta before and after treatment against the background of intravenous administration of a 0.1% Iso-ket solution. The rate of administration of isosorbide dinitrate was titrated according to the rate of decrease in sitolytic blood pressure (not lower than 90 mmHg). The results of the study are presented in Table 2.
Table 2.
Indicators of central hemodynamics in patients with AMI before and after treatment
| Central hemodynamics | Before treatment | Isoket 0.1% solution |
| Treatment time (hours) | 2,97±0,11 | |
| Total nitrate dose (mg) | 29,38+1,39 | |
| Heart rate per minute, p | 114,6+3,13 | 98,38+2,06, <0,01 |
| SI l/min/m2, p | 2,83±0,11 | 2,87+0,09, >0,05 |
| Pressure Pr.Pr mm Hg, p | 8,28±0,57 | 4,82±0,28,<0,001 |
| Average LA pressure, p | 27,7+0,9 | 19,75±0,52,<0,001 |
| DZLA mm Hg, r | 25,6+1,01 | 13,52+0,53,<0,001 |
| LVEDP mm Hg, p | 24,3±1,36 | 9,24+0,55, <0,001 |
| Average pressure Aorta, p | 98,7±1,41 | 90,76+1,65, <0,01 |
As can be seen from the table, in the whole group after intravenous infusion, on average 29.38 + 1.39 mg, Isoket 0.1%, there was a decrease in pressure in the right atrium (preload for the right ventricle) by 41.8%, the average pressure in the pulmonary artery (afterload for the right ventricle) - by 28.7%, PAWP (preload for the left ventricle) - 47.2%, mean pressure in the aorta (afterload for the left ventricle) - by 8.1%. A decrease in pre- and after-loads for both ventricles of the heart contributed to a decrease in PMO2, which was clinically manifested by the relief of pain and cardiac arrhythmias.
Silent and symptomatic episodes of ischemia most often occur in the early morning hours, particularly within two hours of awakening (Figure 3). The risk of developing health-threatening heart disease (acute coronary syndrome, myocardial infarction, sudden cardiogenic death) is not distributed evenly over 24 hours. The frequency of ischemic attacks is noticeably higher in the morning hours from the moment of awakening until noon, with a “plateau” phase during the day and a low level at night.
Rice. 3.
Diagram of the distribution of the frequency of myocardial ischemia and therapeutic concentration in the blood plasma of isosorbide-5-mononitrate when taking Efox-long 50
Taking into account the cyclical nature of cardiogenic events in coronary artery disease, ease of administration (once daily), prevention of the development of tolerance to nitrates, thanks to computer modeling of therapeutic concentration levels and modern drug production technologies, an antianginal drug with biphasic release of the active substance was created and introduced into clinical practice ( Shosorbide-5-mononitrate) - Efox long 50 (Schwarz Pharma). One capsule of Efox Long 50 contains 50 mg of isosorbide mononitrate, which is released in stages as it passes through the gastrointestinal tract with the sequential dissolution of membranes located at different levels inside the capsule (the “matryoshka” principle), which allows it to be used once a day with minimal side effects and maximum clinical effectiveness. The biphasic release of isosorbide mononitrate allows you to quickly achieve a therapeutic effect and continue the antianginal action for a long time: after taking the drug, 30% of the active substance is quickly released, and the remaining 70% is released slowly over 12-19 hours.
To prevent the development of tolerance to nitrates, today it has been proven that it is necessary to adhere to a regimen of taking organic nitrates that would ensure the absence of nitrates in the blood for at least 10 hours. This can be achieved if the prolonged forms are taken once a day, and the regular ones - 2 times in the first half of the day. The need for such a regime has been convincingly demonstrated in a number of studies using retarded forms of isosorbide dinitrate and isosorbide-5-mononitrate.
The effectiveness of isosorbide dinitrate and isosorbide-5-mononitrate in the treatment of angina at rest and exertion has been demonstrated using paired bicycle ergometer tests and cuff techniques in assessing endothelium-dependent responses using two-dimensional ultrasound scanning of the brachial artery.
According to the cuff test during treatment with isosorbide-5-mononitrate, by the end point of the study (3 months) there was a significant increase in the diameter of the brachial artery by 11.6% and an increase in blood flow velocity in the phase of reactive hyperemia by 10.2%, the ratio of flow-dependent to flow-independent vasodilation by during treatment increased from 0.67 to 0.91. At the same time, there was a decrease in the frequency of angina attacks by 80% with an increase in tolerance to physical activity (increase in threshold power by 28% and exercise time by 30%).
A number of other studies, when reproducing myocardial ischemia using the method of paired VEM tests, documented a significant increase in exercise tolerance, a decrease in the frequency of angina attacks and the need for nitroglycerin during treatment with retard forms of isosorbide-5-mononitrate.
All studies noted good patient tolerance of the use of various dosage forms of isosogr-bid-5-mononitrate - a low frequency of negative side effects (Fig. 4).
Rice. 4.
Diagram of the incidence of adverse effects when taking isosorbide-5-mononitrate
The use of organic nitrates, in particular retard forms - Efox-long 50, in the treatment of coronary artery disease (angina at rest and exertion) to prevent the development of ACS, seems to be the most preferable. The duration of the therapeutic effect of Efox-long 50 is determined by its original pharmacokinetics. Standard dosage forms of isosorbide-5-mononitrate, 20 and 40 mg, are prescribed 1 or 2 times during the day, depending on the time and frequency of myocardial ischemia attacks.
The half-life of conventional isosorbide 5-mononitrate tablets is about 6 hours, and the antianginal effect lasts up to 12 hours. The retard form of Efox-long 50, when taken one capsule in the morning, provides a therapeutic concentration in the blood plasma for 12-18 hours and a virtual absence of the drug in the blood (low concentration) during the night, which prevents the development of tolerance to the drug and is well tolerated patients.
Thus, according to the recommendations of the American College of Cardiology/American Heart Association, intravenous administration of nitrates should be a mandatory method of treatment for patients with anterior localization of myocardial infarction. Nitrates for the treatment of AMI can be nitroglycerin (iv infusion - 5 mcg/min) or isosorbide dinitrate (1-2 mg/hour).
Intravenous administration of nitrates in the first 12 hours of MI development helps to reduce the zone; necrosis of the heart muscle, improving the pumping activity of the heart, reducing the incidence of complications and sudden coronary death.
Myocardial infarction. A.M. Shilov
Published by Konstantin Mokanov